TL;DR: A 2026 randomized study in Psychological Medicine found that right orbitofrontal cortex repetitive transcranial magnetic stimulation (rTMS), a noninvasive brain-stimulation method, improved visuospatial memory on the Brief Visuospatial Memory Test-Revised (BVMT) in people with first-episode schizophrenia.
Key Findings
- The analysis included 90 patients: Researchers studied 48 people assigned to active rTMS and 42 assigned to sham stimulation after protocol and cognitive-assessment exclusions.
- All participants received olanzapine: Both groups took olanzapine at 10-20 mg/day, so the comparison tested add-on right OFC rTMS rather than rTMS alone.
- Only visuospatial memory showed a treatment-specific effect: BVMT scores had a significant Time x Group interaction (F = 5.079, p = 0.027, partial eta squared = 0.058).
- The active group improved on BVMT: Post hoc testing showed significant BVMT improvement after active rTMS (p = 0.0007), while the sham group did not show a significant change.
- Symptoms were also lower after active rTMS: At week 4, PANSS total scores were lower in the active group than the sham group (58.9 vs 67.3).
Source: Psychological Medicine (2026) | Hu et al.
Repetitive transcranial magnetic stimulation uses magnetic pulses outside the skull to alter activity in targeted brain networks. In schizophrenia research, rTMS is usually studied as an add-on treatment, not as a replacement for antipsychotic medication.
The new analysis focused on the right orbitofrontal cortex (OFC), a prefrontal region involved in reward processing, decision-making, contextual learning, and links between emotion and cognition.
The target is relevant because cognitive impairment often appears early in schizophrenia and can shape long-term function even when psychotic symptoms improve.
Right OFC rTMS Was Added to Olanzapine Treatment
Researchers analyzed a randomized controlled trial at Shanghai Mental Health Center. The participants had first-episode schizophrenia, were ages 18-45, and were drug-naive before treatment.
The final cognitive analysis included 90 patients. The active group had 48 patients, and the sham group had 42 patients.
The treatment setup was tightly defined:
- Medication background: Every participant stayed on olanzapine at 10-20 mg/day during the treatment period.
- Stimulation target: Active stimulation was delivered over the right OFC, using the AF8 scalp position as the target site.
- Dose schedule: Participants received 20 sessions over 4 weeks, with 5 sessions each week.
- Pulse protocol: Each active session used 1 Hz stimulation at 110% of motor threshold, for 720 pulses per session.
The sham coil matched the active procedure in appearance, weight, and clicking sound but did not produce a magnetic field. Separate blinded teams handled assessment and stimulation procedures.
MCCB Testing Covered Nine Cognitive Measures
Cognition was measured with the MATRICS Consensus Cognitive Battery (MCCB), a standardized set of cognitive tests used in schizophrenia research.
The main outcome was not a broad “thinking” score. Researchers examined 9 separate tests, including processing speed, verbal learning, spatial span, mazes, visual memory, category fluency, emotional intelligence, and sustained attention.
Several measures improved over time when both groups were pooled. Pooled improvement needs caution because it can come from practice effects, natural recovery, symptom reduction, medication effects, or the structure of inpatient treatment.
The stronger test was the Time x Group interaction. That analysis asked whether the active rTMS group changed differently from the sham group.
BVMT Visuospatial Memory Was the Specific Cognitive Signal
The clearest cognitive result came from the Brief Visuospatial Memory Test-Revised (BVMT), which asks participants to remember and reproduce visual designs and their spatial arrangement.
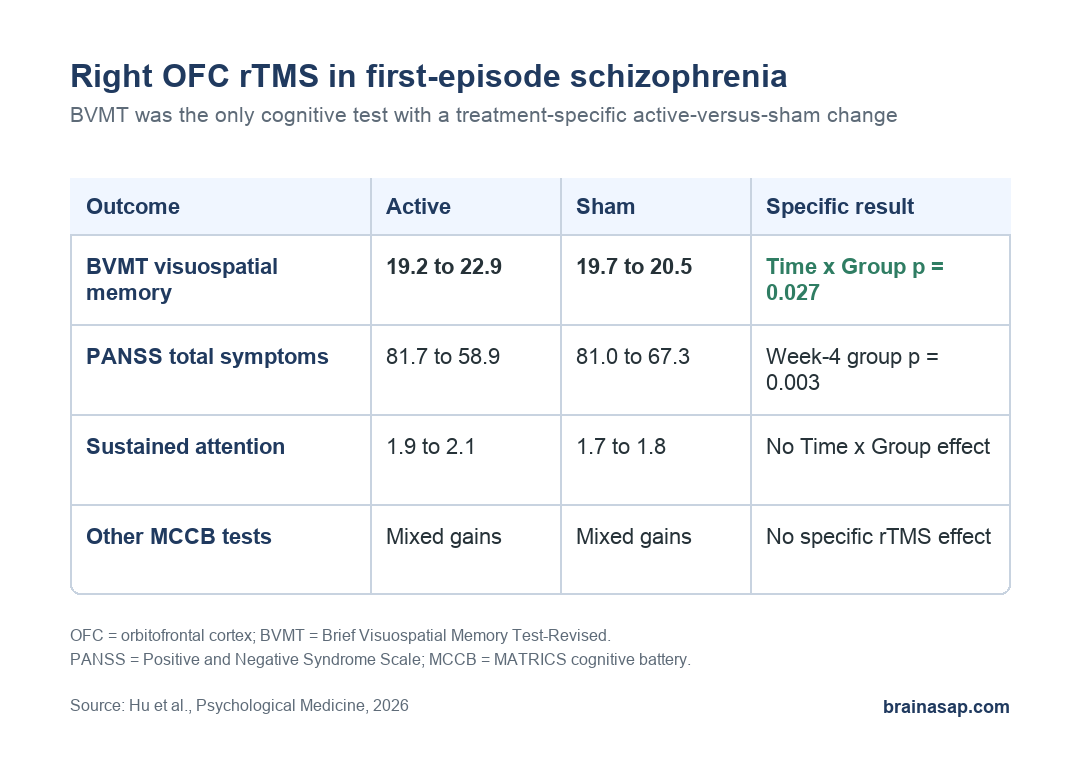
BVMT scores showed a significant Time x Group interaction: F = 5.079, df = 1 and 83, p = 0.027, with partial eta squared = 0.058. By the researchers’ own benchmarks, that effect size was close to medium.
Post hoc tests made the direction easier to read. The active group improved significantly on BVMT, while the sham group did not.
- Active rTMS: BVMT increased from 19.2 to 22.9, with p = 0.0007 in the within-group comparison.
- Sham stimulation: BVMT changed from 19.7 to 20.5 and was not statistically significant.
- Between-group week-4 comparison: Active and sham BVMT scores at week 4 did not differ significantly by simple group comparison, which is why the interaction analysis is the main result.
No other cognitive test showed the same treatment-specific interaction. Trail Making, symbol coding, verbal learning, spatial span, mazes, category fluency, emotional intelligence, and sustained attention did not show significant Time x Group effects.
Symptom Scores Were Lower After Active Stimulation
Psychiatric symptoms were measured with the Positive and Negative Syndrome Scale (PANSS), a 30-item schizophrenia symptom scale covering positive symptoms, negative symptoms, and general psychopathology.
At baseline, the active and sham groups were similar in PANSS scores. After 4 weeks, the active group had lower symptom scores on several PANSS measures.
- PANSS total: 58.9 in the active group versus 67.3 in the sham group (p = 0.003).
- PANSS negative symptoms: 16.2 versus 19.0 (p = 0.012).
- PANSS general psychopathology: 30.2 versus 34.2 (p = 0.001).
- PANSS positive symptoms: 12.5 versus 14.0, a trend that did not reach conventional significance (p = 0.098).
Within the active group, BVMT improvement correlated with lower PANSS total and general psychopathology scores after correction for multiple testing. That does not prove cognition improved because symptoms improved, or the reverse.
It does show that the cognitive and symptom changes moved together in the active-stimulation group more than in the sham group.
The OFC Target Points to a Memory-Network Hypothesis
The OFC is not usually discussed as a simple memory-storage area. Its relevance comes from how it helps connect context, reward, emotional salience, and behavioral choice.
Researchers interpreted the BVMT result as a possible network effect involving OFC connections with hippocampal and parietal systems. That interpretation is plausible, but it should stay secondary to the measured result.
The measured result was narrower: right OFC rTMS improved one visual-memory measure more than sham stimulation over the study window.
That specificity is clinically important. It argues against describing OFC rTMS as a broad cognitive enhancer based on this dataset.
Several Limits Keep the Finding Preliminary
The study was randomized and sham-controlled, but the cognitive analysis still has boundaries a reader should keep visible.
- Olanzapine was present in both groups: Medication could contribute to symptom and cognitive changes, even though dosage did not differ significantly between groups.
- The analyzed sample was modest: Attrition left 48 active and 42 sham participants for the final cognitive analysis.
- Blinding was not formally tested: The procedure was designed to blind participants and evaluators, but the researchers did not report a formal blinding-success check.
- Follow-up was short: Cognitive outcomes were assessed at baseline and week 4, so durability at 3, 6, or 12 months remains unanswered.
Future trials should test right OFC rTMS as an add-on cognitive intervention in first-episode schizophrenia, especially for visuospatial memory.
It is not yet evidence that the same protocol produces broad cognitive recovery, works without antipsychotic treatment, or has durable benefits beyond the short follow-up window.
Citation: DOI: 10.1017/S0033291726103912. Hu et al. The effects of rTMS over orbitofrontal cortex on cognitive functions in first-episode schizophrenia. Psychological Medicine. 2026;56:e119.
Study Design: Secondary cognitive analysis of a randomized sham-controlled rTMS trial in first-episode schizophrenia.
Sample Size: 90 drug-naive patients in the final cognitive analysis; 48 received active right OFC rTMS and 42 received sham stimulation.
Key Statistic: BVMT visuospatial-memory scores showed a significant Time x Group interaction (F = 5.079, p = 0.027, partial eta squared = 0.058).
Caveat: All participants received olanzapine, the sample was modest, blinding success was not formally assessed, and cognitive follow-up ended at 4 weeks.