TL;DR: A 2026 medRxiv preprint linked pre-surgery diffusion MRI markers in Parkinson’s disease to 6-month changes in impulsive-compulsive behaviour after subthalamic deep brain stimulation.
Key Findings
- Small DBS cohort: Researchers followed 35 Parkinson’s disease patients from preoperative diffusion MRI to 6-month clinical follow-up after subthalamic deep brain stimulation.
- Behaviour score: Impulsive-compulsive behaviour was measured with QUIP-RS, a Parkinson’s rating scale for gambling, buying, sexual behaviour, eating, punding, hobbyism, and compulsive medication use.
- Whole cohort stayed mixed: Mean QUIP-RS total score did not significantly change across all 35 patients, moving from 17.9 to 19.0 at 6 months.
- Symptomatic subgroup improved: Among 15 patients with clinically relevant preoperative impulse-control symptoms, QUIP-RS total score improved from 32.5 to 23.7.
- Imaging marker: White-matter microstructure in frontolimbic tracts, including the cingulum and insula-linked pathways, tracked who showed larger behavioural improvement.
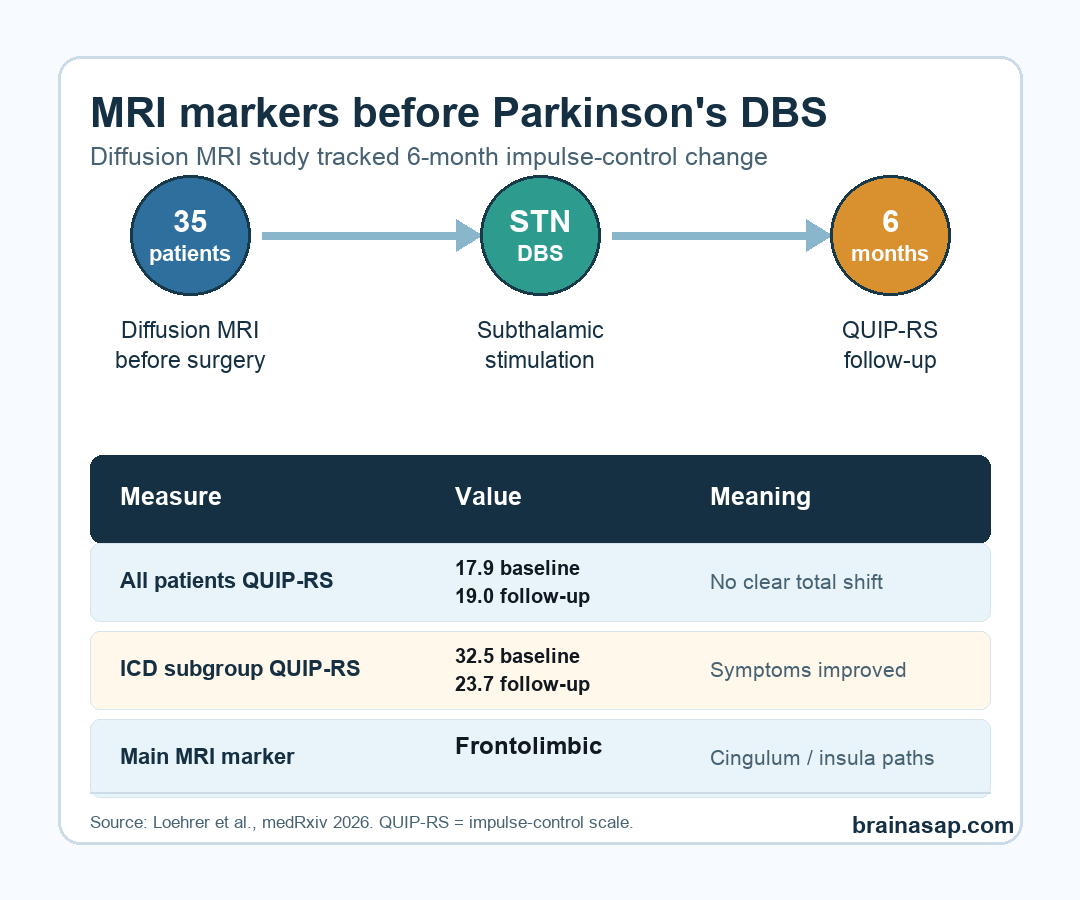
Source: Loehrer et al. medRxiv. 2026.
Diffusion MRI Was Tested Before Parkinson’s DBS Surgery
Subthalamic deep brain stimulation, or STN-DBS, is used for advanced Parkinson’s disease when medication no longer controls motor symptoms well enough.
The stimulation target is motor-focused, but the same brain networks also sit near circuits involved in motivation, reward, and behavioural control.
Impulse-control outcomes are complicated after DBS. Some patients improve after surgery, often as dopamine agonist medication is reduced.
Others develop or worsen impulsive-compulsive behaviours, which can include gambling, compulsive buying, hypersexuality, binge eating, punding, hobbyism, or compulsive medication use.
Researchers asked whether preoperative diffusion MRI could help explain this variation. Diffusion MRI tracks how water movement behaves in tissue, and it can be used to estimate microstructural features of white-matter tracts and grey-matter regions before surgery.
The key idea is not that an MRI scan “sees” impulsivity. Frontolimbic circuits, the pathways connecting frontal control regions with emotion and reward systems, may shape how the brain responds when stimulation and medication changes happen together.
The Study Followed 35 Patients for 6 Months
The study enrolled people with Parkinson’s disease who were already candidates for DBS surgery. After 2 exclusions for missing follow-up data, the analysis included 35 patients.
Their average age was 58.7 years, and average disease duration was 8.9 years. The cohort was a small but clinically relevant advanced-Parkinson’s surgical sample, not a general population aging sample.
Clinical assessments were done before surgery and again at 6 months. Baseline testing was performed in the ON-medication state, meaning usual Parkinson’s medication was active, while follow-up testing was performed with medication and stimulation active.
- Behaviour outcome: The main scale was QUIP-RS, short for Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease-Rating Scale.
- Quality of life: Researchers also measured PDQ-8 summary index, an 8-item Parkinson’s quality-of-life score.
- Medication exposure: They tracked levodopa equivalent daily dose, including dopamine agonist dose.
The imaging side used diffusion tensor imaging and NODDI, short for neurite orientation dispersion and density imaging. Researchers tested diffusion microstructure markers across the brain instead of relying on a narrow MRI summary.
Those markers included fractional anisotropy, mean diffusivity, neurite density index, and orientation dispersion index. The team used multiple diffusion-derived measures to ask whether baseline tissue organization was tied to later behavioural change.
Whole-Group Impulse Scores Did Not Shift Much
Across all 35 patients, total QUIP-RS did not significantly change from baseline to 6 months. Mean total score moved from 17.9 to 19.0, with p=.94 and Cohen’s d=-.07.
The whole-group null result keeps the claim narrow. The researchers are not saying DBS broadly cured or worsened impulse-control symptoms in the full cohort.
Instead, the main point was about which baseline brain microstructure patterns were associated with better or worse 6-month behavioural change.
Other outcomes did improve. PDQ-8 quality-of-life summary score fell from 32.9 to 22.2. Total levodopa equivalent daily dose fell from 965.4 mg to 543.5 mg, and dopamine agonist-equivalent dose also dropped.
The medication drop is clinically important. Dopamine agonists can contribute to impulse-control symptoms in some Parkinson’s patients, so a post-DBS behavioural change can reflect a mix of brain stimulation, dopamine agonist reduction, and the patient’s preexisting circuit vulnerability.
Patients With Clinically Relevant ICDs Improved More
A subgroup of 15 patients had clinically relevant preoperative impulse-control symptoms. In that group, QUIP-RS total score improved from 32.5 to 23.7 at 6 months, with p=.003 and Cohen’s d=.71.
The strongest subscore changes were narrower than the total behaviour scale. They appeared in 2 compulsive behaviour domains:
- Hobbyism: The subgroup mean moved from 6.4 to 4.3, with p=.018.
- Punding: The subgroup mean moved from 5.1 to 2.7, with p<.001.
- Medication context: Dopamine agonist dose reduction is a plausible contributor, so the behavioural improvement should not be read as a stimulation-only effect.
The subgroup result also helps explain why a simple whole-cohort average can miss the clinical pattern. Patients who entered surgery with clinically relevant symptoms had more room to improve, while patients without those symptoms could remain stable or shift in either direction.
Frontolimbic White Matter Carried the Cleaner Signal
The imaging results were anatomical rather than single-score simple. Higher fractional anisotropy in the left cingulum was associated with greater postoperative reduction in QUIP-RS.
The cingulum is a white-matter tract tied to attention, emotion, memory, and control networks. In this study, the tract helped anchor the broader frontolimbic interpretation.
Other diffusion measures pointed in a similar frontolimbic direction. Lower orientation dispersion index in regions around the cingulum, insula-linked white matter, uncinate fasciculus, superior longitudinal fasciculus, and frontal-orbital connections was associated with larger reductions in impulsive-compulsive symptoms.
The insula-linked findings are especially plausible because the insula helps integrate body state, salience, urge, and decision-making signals. The cingulum finding also fits a control-network interpretation, because this tract connects regions involved in monitoring behaviour and adjusting actions.
- White-matter tract pattern: Some frontolimbic and association pathways looked linked to better 6-month behavioural outcomes.
- Grey-matter contrast: Intact microstructure in areas such as paracingulate gyrus, insular cortex, and precentral gyrus was associated with lower reductions or possible increases in postoperative ICB.
- Clinical interpretation: The result supports risk stratification, not a ready-made individual prediction tool.
The Main Limit Is Early Evidence
This was a prospective open-label study, not a blinded trial built to prove a clinical decision rule. The sample was small, the behavioural outcomes were patient-reported, and the analysis tested complex MRI metrics that need larger validation cohorts.
The source is a medRxiv preprint, meaning the report had not yet completed peer review.
The finding remains informative, but the clinical interpretation should stay cautious.
Diffusion MRI may eventually help identify DBS patients who need closer behavioural monitoring, but it is not yet a stand-alone screening test.
A practical future test would ask whether the same MRI markers predict behavioural outcomes in an independent DBS cohort, ideally with standardized medication-adjustment records and enough participants to separate gambling, buying, eating, sexual behaviour, hobbyism, punding, and medication-use symptoms.
Until then, the clearest use is planning. A patient with a risk-heavy imaging profile would still need ordinary clinical judgment, but the care team might watch impulse-control symptoms more closely during medication reduction and stimulator programming.
Family reports could also matter, because some impulse-control changes are easier for caregivers to notice than for patients during real-world clinical follow-up.
- Best current use: The study gives a mechanistic clue about frontolimbic circuits and postoperative impulse-control risk.
- What clinicians still need: Larger, preregistered, longitudinal validation before using these markers to guide DBS counselling.
- Reader takeaway: The same DBS procedure can improve motor symptoms while behavioural outcomes depend on medication changes, stimulation effects, and each patient’s network anatomy.
Citation: DOI: 10.64898/2026.04.13.26350763. Loehrer et al. Microstructure predicts impulsive and compulsive behaviour following subthalamic stimulation in Parkinson’s disease. medRxiv. 2026.
Study Design: Prospective open-label diffusion MRI study with 6-month DBS follow-up.
Sample Size: 35 Parkinson’s disease patients; 15 had clinically relevant preoperative impulse-control symptoms.
Key Statistic: In the clinically relevant ICD subgroup, mean QUIP-RS total score improved from 32.5 to 23.7 at 6 months.
Caveat: This is a small preprint study, and the MRI markers need validation before they can guide individual DBS decisions.





