TL;DR: A 2026 Neurological Sciences study followed 216 early Parkinson’s patients for 2 years after levodopa started and found that several non-motor symptom differences between men and women persisted or emerged despite adjustment for baseline scores and levodopa dose.
Key Findings
- 216 early Parkinson’s patients completed 24-month follow-up after starting levodopa, including 139 men and 77 women from 17 Italian movement-disorder centers.
- Women had higher anxiety and pain scores at baseline and again at 24 months, even after the follow-up analysis adjusted for baseline scores and levodopa dose.
- Women also had worse mobility and emotional well-being on the PDQ-39 quality-of-life questionnaire at both time points.
- Men had higher hypersexuality scores at 24 months on the Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease (QUIP).
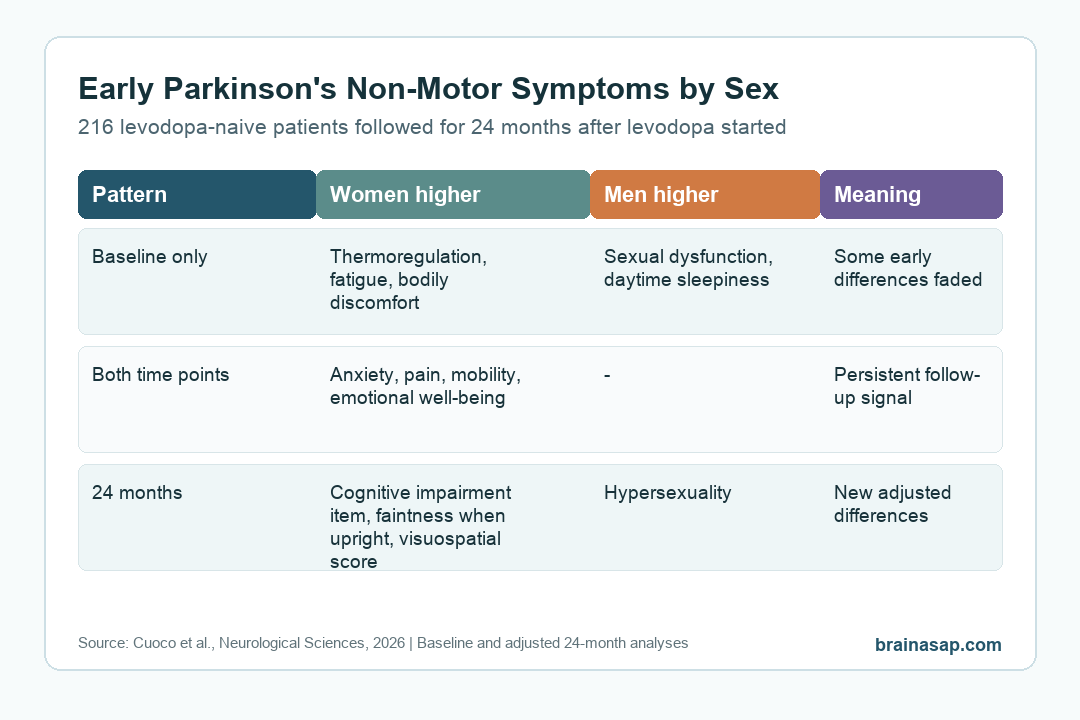
- Some early differences disappeared after 2 years, including baseline differences in thermoregulation, fatigue, daytime sleepiness, sexual dysfunction, and bodily discomfort.
Source: Neurological Sciences (2026) | Cuoco et al.
Researchers Followed Levodopa-Naive Parkinson’s Patients for 2 Years
Non-motor symptoms are not side issues in Parkinson’s disease. Anxiety, pain, autonomic symptoms, sleepiness, fatigue, impulse-control symptoms, and cognitive changes can shape daily life as much as tremor or slowness.
This study focused on an early point in the disease course. Researchers enrolled levodopa-naive Parkinson’s patients before their initial levodopa dose, then reassessed them after 24 months of treatment and follow-up.
The final cohort included 216 people: 139 men and 77 women. The study was multicenter, drawing from 17 Italian movement-disorder centers, which makes the sample broader than a single-clinic case series.
The central question was practical: do men and women show different non-motor symptom profiles early in Parkinson’s disease, and do those differences still matter after levodopa begins?
- Baseline comparison: researchers compared men and women before levodopa initiation.
- Follow-up comparison: researchers tested 24-month outcomes with analysis of covariance, adjusting for baseline scores and levodopa dose at follow-up.
- Symptom coverage: the study included autonomic symptoms, mood, cognition, quality of life, impulse-control symptoms, apathy, and Parkinson’s non-motor scales.
Anxiety, Pain, Mobility, and Emotional Well-Being Stayed Higher in Women
The clearest repeated pattern involved anxiety, pain, mobility, and emotional well-being.
At baseline, women scored higher than men on anxious mood, pain and other sensations, PDQ-39 mobility, and PDQ-39 emotional well-being.
Those differences were still present at 24 months. After adjustment, women had higher mean scores for UPDRS Part I anxious mood (1.03 vs 0.61), pain and other sensations (0.86 vs 0.58), PDQ-39 mobility (8.26 vs 4.17), and PDQ-39 emotional well-being (5.79 vs 3.42).
These are group averages, not individual predictions. The persistence after adjustment matters because the 24-month analysis controlled for where patients started and for levodopa exposure.
In clinical terms, these findings support asking directly about anxiety, pain, and quality-of-life burden during early Parkinson’s visits.
Those symptoms may be part of a sex-specific non-motor pattern that is visible near treatment initiation and still measurable 2 years later.
Men Had Higher Hypersexuality Scores at 24 Months
The male-skewed result at follow-up involved hypersexuality, an impulse-control symptom measured with QUIP, the Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease.
At 24 months, men had higher hypersexuality scores than women (1.88 vs 0.50, p < 0.001).
This finding fits a known clinical concern in Parkinson’s care: dopaminergic treatment can be associated with impulse-control problems in some patients, and sex can influence how those symptoms show up.
Researchers did not claim that levodopa alone caused this difference. Men also had slightly higher levodopa doses at 24 months (327.64 vs 286.69 mg/day), and the analysis adjusted for levodopa dose.
The result therefore points to a follow-up difference that was not simply explained by the measured dose variable.
- Female-skewed follow-up symptoms: anxiety, pain, mobility burden, emotional well-being burden, cognitive impairment item, feeling faint when upright, and visuospatial performance.
- Male-skewed follow-up symptom: hypersexuality on the QUIP scale.
- Symptoms without follow-up sex difference: many autonomic, sleep, urinary, gastrointestinal, apathy, and depression-scale measures did not remain significantly different.
Some Baseline Differences Did Not Persist
Several differences were visible at baseline but were no longer significant after 2 years.
This split separates early symptom-profile differences from differences that appear more durable.
At baseline, women had higher cardiovascular and thermoregulatory autonomic scores, higher fatigue, and higher bodily discomfort. Men had higher sexual dysfunction and daytime sleepiness.
These differences were not the main 24-month pattern after adjustment.
The study authors interpret this cautiously. Disease duration, treatment exposure, and symptom progression may change which sex-related differences remain detectable.
A baseline difference is still clinically useful, but it should not be assumed to predict the same group difference 2 years later.
- Persistent areas: anxiety, pain, mobility, and emotional well-being were different at both baseline and follow-up.
- Follow-up-emerging areas: hypersexuality, cognitive impairment item, feeling faint when upright, and visuospatial performance showed significant 24-month differences.
- Fading areas: fatigue, daytime sleepiness, sexual dysfunction, thermoregulation, and bodily discomfort were baseline differences that did not persist in the adjusted follow-up analysis.
What the Study Means for Early Parkinson’s Care
Early Parkinson’s care needs broad non-motor screening rather than a narrow motor checklist.
Clinicians need to ask directly about symptoms that patients may not volunteer on their own.
For women with early Parkinson’s disease, the study supports careful attention to anxiety, pain, mobility burden, emotional well-being, orthostatic symptoms, and visuospatial cognition. For men, impulse-control symptoms such as hypersexuality deserve explicit monitoring during follow-up.
Because this was an observational cohort, the study cannot prove biological causes for the sex differences. Hormonal, genetic, psychosocial, medication-related, and care-access factors could all contribute.
The analysis also lost 69 participants to follow-up, largely because COVID-19 restrictions interfered with study visits.
Even with those limits, the design answers a useful clinical question. In early Parkinson’s disease, non-motor symptoms are already structured by sex in ways that can persist after levodopa starts.
Routine follow-up should look for those symptoms before they quietly become the main source of disability.
Citation: DOI: 10.1007/s10072-026-09031-2. Cuoco et al. Gender differences in non-motor symptoms in Parkinson’s disease: a multicenter longitudinal study. Neurological Sciences. 2026;47:427.
Study Design: Multicenter prospective longitudinal cohort study across 17 Italian movement-disorder centers.
Sample Size: 216 early levodopa-naive Parkinson’s patients completed 24-month follow-up: 139 men and 77 women.
Key Statistic: At 24 months, women had higher anxiety, pain, mobility, and emotional well-being burden, while men had higher QUIP hypersexuality scores.
Caveat: The study was observational, follow-up was affected by COVID-19 restrictions, and group differences do not determine individual symptom profiles.





