TL;DR: A 2026 preprint in medRxiv reported that serum myelin oligodendrocyte glycoprotein (MOG) protein was higher in multiple sclerosis than controls and higher during clinical relapse than remission.
Key Findings
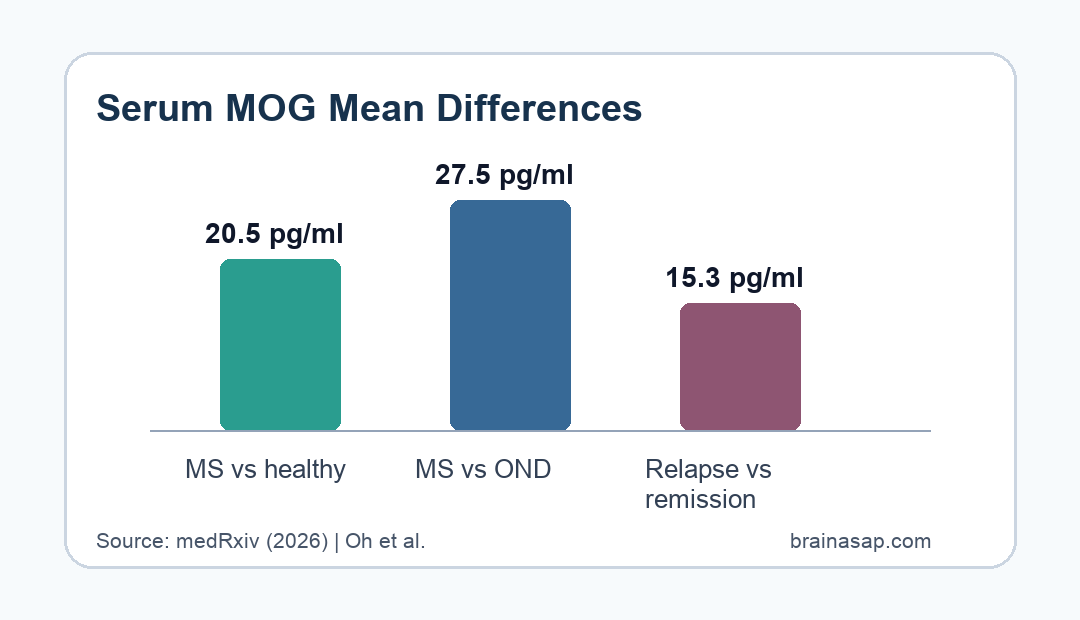
- 20.5 pg/ml higher: Serum MOG protein was higher in MS than healthy donors by a mean difference of 20.5 pg/ml.
- 27.5 pg/ml higher: MS samples were also higher than other neurological disease controls by 27.5 pg/ml.
- 15.3 pg/ml relapse gap: MS relapse samples had higher MOG protein than remission samples by 15.3 pg/ml.
- 0.85 AUC: MOG distinguished MS from healthy donors with an area under the curve (AUC) of 0.85.
- 0.82 AUC: MOG distinguished MS from other neurological disease controls with an AUC of 0.82.
Source: medRxiv (2026) | Oh et al.
Serum MOG protein is different from anti-MOG antibodies. The study measured the MOG protein itself in blood as a possible marker of central nervous system myelin damage in multiple sclerosis (MS).
The preprint’s central claim is that MOG protein may add a demyelination-focused signal alongside neurofilament light chain, a blood marker more closely tied to neuroaxonal injury.
Blood MOG Protein Was Higher in Multiple Sclerosis
Researchers tested treatment-naive relapsing MS samples against two control groups. In the first cohort, MS samples were compared with age-, sex-, and race-matched healthy donors.
Serum MOG was higher in MS than healthy donors by a mean difference of 20.5 pg/ml, with a 95% confidence interval from 12.7 to 28.2 pg/ml.
- Cohort 1: 33 people with relapsing-remitting MS were compared with 35 healthy donors.
- Cohort 2: 30 treatment-naive relapsing MS samples were compared with 42 other neurological disease controls.
- Control diagnoses: The other neurological disease group included headache, dementia, motor neuron disease, neuropathy, and stroke controls.
In the second cohort, serum MOG was also higher in MS than other neurological disease controls by 27.5 pg/ml, with a 95% confidence interval from 17.5 to 40.5 pg/ml.
MOG Protein Also Tracked MS Relapse Versus Remission
The study separately compared MS samples collected during clinical relapse with samples from MS remission. Clinical relapse meant new or recurrent MS symptoms lasting more than 24 hours after at least 30 days of neurologic stability, without fever.
Relapse samples had higher MOG protein than remission samples by a mean difference of 15.3 pg/ml, with a 95% confidence interval from 6.11 to 25.6 pg/ml.
- Relapse group: 35 MS samples were collected during clinical relapse.
- Remission group: 27 MS samples were collected during clinical remission.
- Disease-activity readout: The relapse-remission contrast suggests MOG may reflect active demyelination, not only diagnostic status.
The relapse contrast is the clinically relevant part. A biomarker that rises during relapse could help separate active myelin injury from stable disease, although the study does not establish how it should guide treatment decisions.
The timing definition also matters. Relapse was not treated as any symptom fluctuation; it required new or recurrent symptoms lasting more than 24 hours, preceding neurologic stability, no fever, and examination-based functional-system change.
That definition makes the relapse-remission comparison more interpretable than a simple self-report contrast. It still does not prove that MOG predicts relapse before symptoms, but it supports testing MOG in future longitudinal monitoring studies.
MOG Added Information Beyond Neurofilament Light Chain
The researchers also measured neurofilament light chain (NfL), a marker of neuroaxonal injury. MOG and NfL were moderately correlated, but the preprint reports that MOG added information about disease activity not captured by NfL alone.
The receiver operating characteristic results showed good discrimination for MOG. MOG had an AUC of 0.85 for MS versus healthy donors and 0.82 for MS versus other neurological disease controls.
- MOG focus: MOG is a myelin protein enriched in the outer myelin sheath.
- NfL focus: NfL reflects axonal injury rather than myelin-specific damage.
- Combined value: A demyelination marker and an axonal-injury marker may describe different parts of MS activity.
That distinction is biologically useful because MS lesions involve both demyelination and axonal injury. A single blood marker may not capture both processes equally well.
The preprint also tested sample stability through repeat freeze-thaw cycles in a small donor set. Up to three freeze-thaws did not significantly change measured MOG protein levels, which is relevant for stored biobank samples.
Assay reliability is not the same as clinical validity, but it affects whether a candidate biomarker can be studied across archived samples. If the protein were unstable after routine handling, the diagnostic and relapse findings would be harder to interpret.
The Preprint Needs Peer Review and Clinical Validation
The evidence is promising, but it should not be treated as a clinical test yet. The source is a medRxiv preprint, and the paper itself states that it has not been certified by peer review and should not guide clinical practice.
The cohorts were also modest in size, and the second control cohort was not perfectly matched to the MS group. Larger, prospective studies would need to test timing, thresholds, treatment effects, MRI lesion activity, and relapse prediction.
- Strength: The study used independent diagnostic comparison cohorts and a relapse-remission analysis.
- Limit: Blood MOG protein still needs validation across MS subtypes, treatments, and longitudinal follow-up.
- Clinical question: The next issue is whether MOG changes before relapse, during MRI activity, or after treatment response.
For now, the cleanest interpretation is that serum MOG protein may be a candidate blood marker for MS demyelination and activity, not a ready replacement for clinical examination, MRI, or established laboratory context.
Citation: DOI: 10.1101/2025.09.06.25335236. Oh et al. Serum myelin oligodendrocyte glycoprotein as an indicator of diagnosis and disease activity in multiple sclerosis. medRxiv. 2026.
Study Design: Preprint case-control biomarker study of serum MOG protein in MS, controls, relapse, and remission.
Sample Size: 33 MS versus 35 healthy donors; 30 MS versus 42 other neurological disease controls; 35 relapse versus 27 remission samples.
Key Statistic: Serum MOG was 15.3 pg/ml higher in MS relapse than remission and had AUC 0.82 for MS versus other neurological disease controls.
Caveat: This is a non-peer-reviewed preprint, so the findings should not guide clinical practice without validation.





