TL;DR: A 2026 medRxiv preprint found that older adults with Montreal Cognitive Assessment (MoCA)-defined mild cognitive impairment had less coordinated pulse-wave responses during a cognitive challenge than cognitively intact older adults.
Key Findings
- Community cognitive-aging sample: The southern Taiwan dataset included 101 older adults: 12 reference participants, 50 people in a MoCA-defined mild cognitive impairment stratum, and 39 people in a dementia-level MoCA stratum.
- 55 paired recordings: Task-evoked pulse-wave analyses used 10 reference participants and 45 MCI participants after missing or low-quality recordings were excluded.
- MoCA-defined groups: Mild cognitive impairment was defined by MoCA scores of 18 to 25; the labels were screening strata, not confirmed clinical diagnoses.
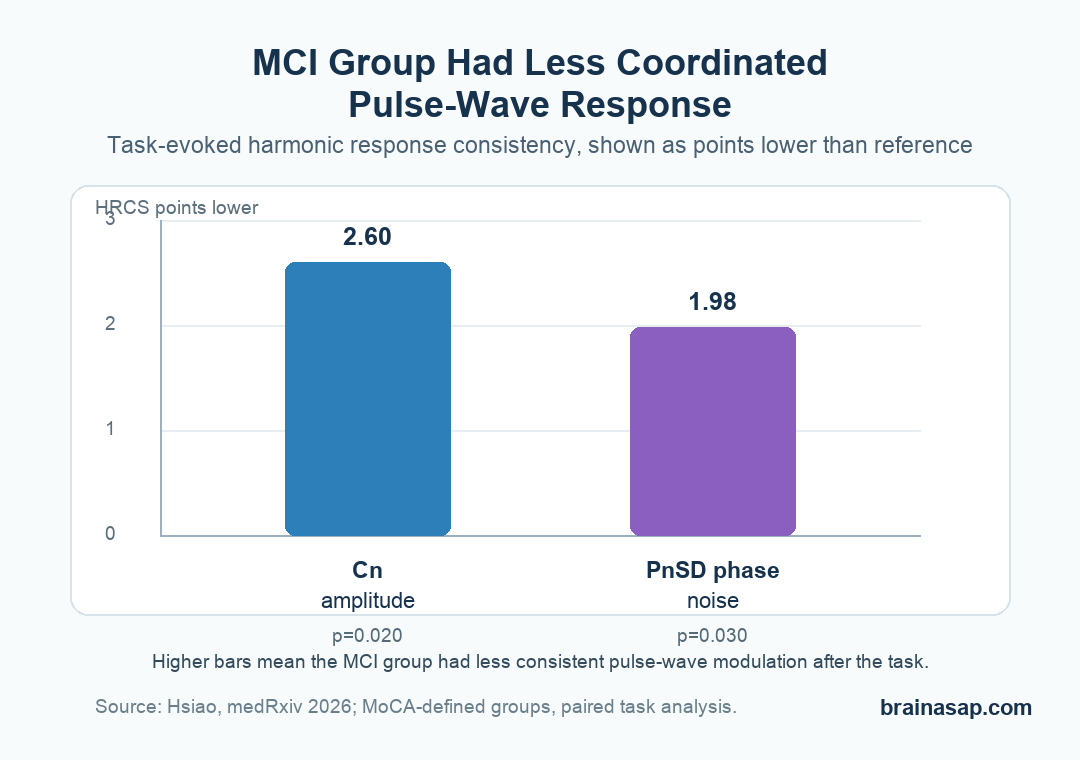
- Amplitude coherence was lower: The MCI group had lower harmonic response consistency in the Cn amplitude domain, with a mean difference of 2.60 points.
- Phase-noise coherence also differed: The MCI group also showed lower consistency in the PnSD phase-noise domain, with a mean difference of 1.98 points.
Source: medRxiv preprint (2026) | Hsiao
Pulse waves are not brain measurements. They are pressure-wave patterns shaped by the heart, blood vessels, and autonomic regulation.
This study asked whether those patterns become more informative when older adults are given a short cognitive challenge.
A pulse recording did not diagnose mild cognitive impairment. The measured difference was that pulse-wave organization during the task looked more coordinated in cognitively intact older adults and more fragmented in the MoCA-defined MCI group.
Pulse-Wave Harmonics Were Tested During a Cognitive Task
The study used a community-based cross-sectional design in southern Taiwan. Participants were older adults who completed cognitive screening, health questionnaires, blood pressure measures, laboratory tests, and pulse-wave recordings.
Cognitive status was grouped by Montreal Cognitive Assessment (MoCA) score. MoCA is a brief cognitive screening test, not a full diagnostic workup.
The reference group scored 26 or higher, the MCI stratum scored 18 to 25, and the dementia-level stratum scored below 18.
The task-evoked analysis focused on participants with usable pulse recordings before and after the cognitive task. That left 55 paired recordings: 10 in the reference group and 45 in the MCI group.
- Pulse-wave input: The study analyzed harmonic amplitudes and phase-related measures from pulse recordings.
- Cognitive input: A subtraction task served as the acute cognitive challenge.
- Main comparison: The researchers compared response organization in the reference and MCI strata.
- Excluded from task analysis: The dementia-level group was not included in the pre-post cognitive-task comparison.
HRCS Measured Directional Consistency, Not Diagnosis
The central measure was the Harmonic Response Consistency Score (HRCS). It summarized whether the first 10 harmonic orders tended to change in the same direction after the task.
A score of 10 means all 10 harmonics shifted in one consistent direction. A score of 0 means the response was directionally fragmented.
The researchers calculated HRCS separately for harmonic amplitude, variability, phase angle, and phase-noise domains.
Ordinary mean pre-post changes can miss this kind of pattern-level difference. Two people can show small average changes while one has a coordinated response across harmonic orders and the other has a scattered response.
The paper described HRCS as a physiological organization index, not a diagnostic classifier. That distinction should stay visible: the result supports a research signal, not a screening tool ready for clinic use.
Amplitude and Phase-Noise Coherence Were Lower in MCI
The clearest group differences appeared in harmonic amplitude and phase-noise consistency.
In the Cn amplitude domain, the MCI group had lower HRCS values than the reference group, with a mean difference of 2.60 points and a 95% confidence interval from 0.29 to 4.91.
Phase-noise consistency showed a similar pattern. The PnSD domain differed by 1.98 points, with a 95% confidence interval from 0.04 to 3.92.
The reference group showed high response consistency, with mean HRCS around 9.00. The paper described this as coordinated harmonic down-modulation after the cognitive challenge.
By contrast, the MCI group showed more attenuated and directionally mixed responses. The pulse-wave pattern changed less like one organized system and more like a set of partly disconnected responses.
- Cn amplitude domain: Lower consistency in the MCI group suggested weaker coordinated amplitude modulation.
- PnSD phase-noise domain: Lower consistency suggested less stable phase-noise organization during cognitive demand.
- Pn phase angle domain: The group difference was not statistically significant.
- CVn variability domain: The group difference was also not statistically significant.
Resting Pulse Measures Were Less Directly Cognitive
The baseline pulse-wave findings were more limited. Resting harmonic features were only weakly related to cognitive and psychological measures, with significant correlations mainly involving lower-order harmonics and systolic blood pressure.
Resting pulse-wave data mostly reflected vascular-regulatory state, not cognitive performance by itself.
The cognitive task changed the interpretation. Under challenge, the organization of the response became the more useful readout.
The study therefore points toward regulatory flexibility, not a static pulse biomarker.
A body-wide physiological system may reveal more when it is mildly stressed than when it is measured at rest.
That does not make the pulse wave a dementia test, but it gives researchers a noninvasive measure to study alongside cognitive screening.
The Small Reference Group Limits the Claim
The study has several hard boundaries. The task-evoked comparison relied on only 10 reference participants, while the MCI group had 45.
The cognitive strata also differed by age and education, which can affect both MoCA performance and cardiovascular physiology.
The design was cross-sectional, so it cannot show whether fragmented pulse-wave responses predict later cognitive decline. The paper also used one subtraction task, not a broad battery of cognitive demands.
- Screening labels: MoCA strata do not equal full clinical diagnoses of MCI or dementia.
- Demographic imbalance: Age and education differed across cognitive groups.
- Small reference group: The paired reference sample had only 10 usable participants.
- Preprint status: The report has not yet been certified by peer review.
The paper did not claim that pulse-wave harmonics diagnose MCI.
It showed that a cognitive task exposed differences in cross-harmonic response organization that were not obvious from static averages alone.
The next test would be longitudinal: whether lower HRCS during cognitive challenge predicts later cognitive decline, conversion to dementia, or change on formal neuropsychological testing.
Citation: DOI: 10.64898/2026.04.24.26351647. Hsiao K-Y. Pulse-wave harmonic signatures of cardiovascular regulatory coherence to a cognitive challenge in mild cognitive impairment: a community-based cross-sectional study. medRxiv. 2026.
Study Design: Community-based exploratory cross-sectional study with within-session pre-post cognitive-task pulse recordings.
Sample Size: 101 older adults overall; task-evoked paired analyses used 10 reference participants and 45 MoCA-defined MCI participants.
Key Statistic: MCI participants had lower HRCS than reference participants in the Cn amplitude domain, mean difference 2.60 (95% CI: 0.29 to 4.91).
Caveat: This is a non-peer-reviewed preprint with a small reference group, demographic imbalance, and MoCA-defined cognitive strata rather than confirmed diagnoses.





