TL;DR: A 2026 MRI preprint on medRxiv found that patients with catatonia were less likely to have a left paracingulate sulcus (PCS), a stable anterior cingulate cortex fold, than psychiatric patients without catatonia.
Key Findings
- 523 MRI scans: Researchers compared 109 patients with catatonia, 323 psychiatric patients without catatonia, and 91 healthy controls.
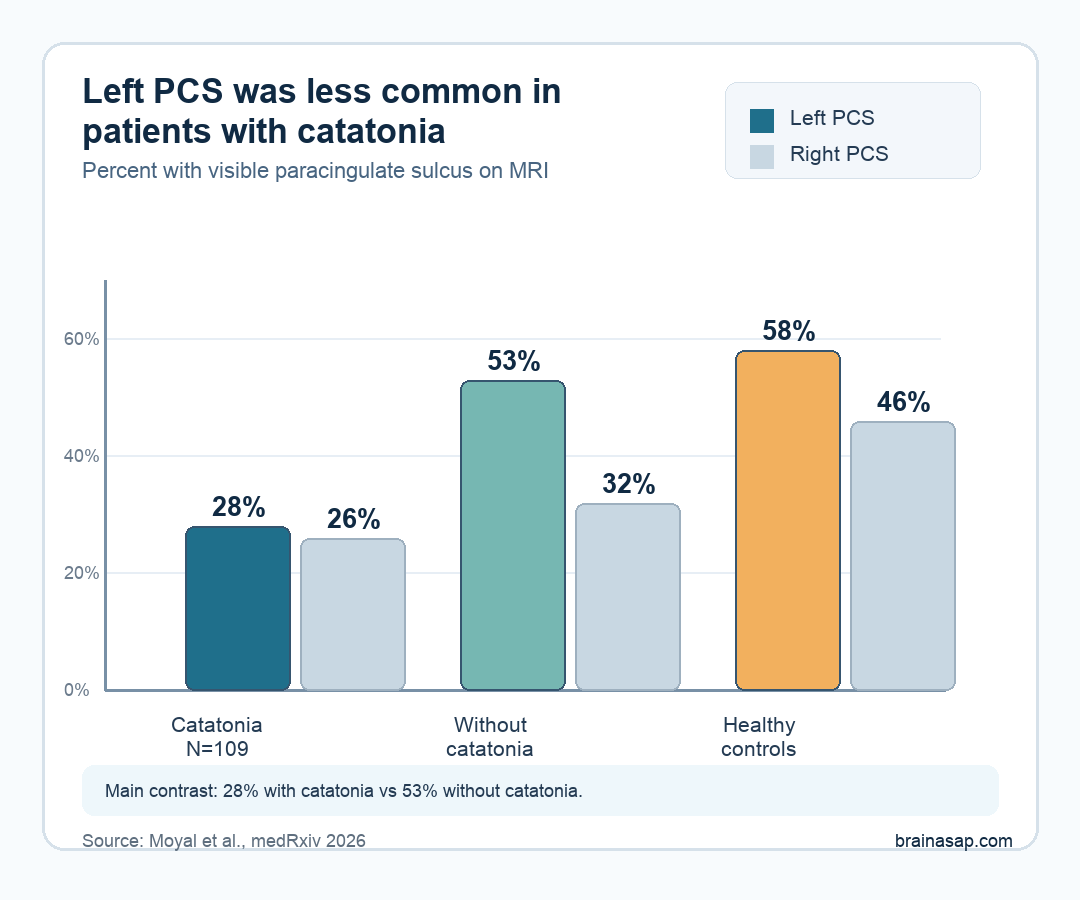
- Left PCS was less common: A visible left paracingulate sulcus appeared in 28% of the catatonia group versus 53% of psychiatric patients without catatonia.
- Right PCS did not show the same result: Right-side PCS presence was 26% with catatonia, 32% without catatonia, and 46% in controls, but the adjusted right-side model was not significant.
- The signal crossed diagnoses: The left-side pattern was seen across psychotic and mood-disorder contexts, supporting catatonia as a transdiagnostic syndrome rather than only a schizophrenia feature.
- Severity was not explained: Among catatonia patients with Bush-Francis Catatonia Rating Scale scores, PCS pattern did not track current catatonia severity.
Source: medRxiv preprint (2026) | Moyal et al.
Catatonia is a severe psychomotor syndrome involving symptoms such as stupor, mutism, posturing, waxy flexibility, agitation, negativism, and abnormal movement initiation. It can appear in schizophrenia, mood disorders, neurodevelopmental conditions, medical illness, and rare genetic syndromes.
The new preprint asked whether catatonia leaves a clue in a brain fold that is set early in development. The focus was the anterior cingulate cortex (ACC), a region involved in motor initiation, cognitive control, and affective integration.
Researchers Compared ACC Folding in Catatonia, Other Psychiatric Patients, and Controls
The study used high-resolution T1-weighted MRI scans from a Paris hospital-based cohort. Researchers screened records from people with schizophrenia-spectrum or mood-spectrum diagnoses and confirmed catatonia by DSM-5 criteria, then compared them with psychiatric patients who had no catatonia history and healthy controls.
The sample had three main groups:
- Catatonia group: 109 patients, including 89 with psychotic disorders and 20 with mood disorders.
- Psychiatric comparison group: 323 patients without catatonia, including 237 with psychotic disorders and 86 with mood disorders.
- Healthy control group: 91 people without a reported psychiatric history.
The central structure was the paracingulate sulcus (PCS), an extra fold that can run near the cingulate sulcus in the anterior cingulate region. Its presence or absence is treated as a stable cortical-folding feature, not a day-to-day symptom marker.
Two blinded raters inspected each hemisphere, and disagreements were resolved with a third rater. Analyses adjusted for age, sex, scanner type, intracranial volume, and medication exposure using olanzapine- and diazepam-equivalent doses.
Left PCS Presence Was Lower in the Catatonia Group
The main result was left-sided. Left PCS was visible in 31 of 109 patients with catatonia, or 28%.
By comparison, it appeared in 171 of 323 psychiatric patients without catatonia, or 53%, and in 53 of 91 healthy controls, or 58%.
The adjusted model found a significant diagnostic-group effect for left PCS presence (chi-square = 16.65, p = .0002).
In post hoc testing, patients with catatonia were significantly less likely to show a left PCS than psychiatric patients without catatonia (p = .0004).
The right hemisphere did not carry the same statistical result. Right PCS was present in 26% of the catatonia group, 32% of the psychiatric comparison group, and 46% of controls, but the adjusted right-side model was not significant.
The Catatonia Pattern Was Not Just a Psychosis Pattern
Catatonia has historically been tied closely to schizophrenia, but modern clinical practice treats it as a syndrome that can cross diagnostic boundaries. This study tested that idea directly by separating psychotic disorders and mood disorders in subgroup analyses.
The left PCS pattern remained most visible in the psychosis subgroup: 27% of psychotic-disorder patients with catatonia had a left PCS versus 49% of psychotic-disorder patients without catatonia.
The adjusted subgroup model again showed a left-side group effect (chi-square = 13.73, p = .003).
For mood disorders, the sample was smaller. Left PCS appeared in 35% of mood-disorder patients with catatonia and 44% of mood-disorder patients without catatonia.
That comparison did not survive as a clear pairwise result, so the mood-disorder finding should be read cautiously.
The broader interpretation is still important. The strongest statistical contrast was not simply “schizophrenia versus everyone else.” It was a catatonia-linked anatomical pattern, especially in left anterior cingulate folding.
Why a Stable Brain Fold Points Toward Vulnerability Rather Than Current Symptoms
Cortical folding develops largely before birth and remains relatively stable after early life. For that reason, researchers interpreted PCS pattern as a possible developmental vulnerability feature.
They did not present it as a marker of whether someone was actively catatonic during the MRI scan.
The distinction matters for clinical interpretation:
- Stable anatomy: A fixed folding feature that may reflect early neurodevelopmental risk.
- Current symptoms: A changing clinical measure that rises or falls with current catatonia severity.
- This study’s result: PCS pattern fit stable vulnerability more closely than current symptom intensity.
The severity analysis supported that interpretation. Among patients with catatonia who had Bush-Francis Catatonia Rating Scale (BFCRS) data, PCS pattern did not correlate with severity.
In plain terms, the fold pattern helped separate groups, but it did not explain who had more intense catatonia symptoms at the measured clinical point.
The ACC also gives the result biological plausibility. The region helps coordinate movement initiation, cognitive control, emotional processing, and fronto-striatal circuits.
Those systems are relevant to catatonia because the syndrome often involves impaired starting, stopping, sustaining, or organizing movement.
The Result Still Needs Prospective Replication
The preprint has several limits. It was retrospective, so MRI timing did not necessarily match an active catatonia episode.
Clinical records may also miss catatonia in some patients, which could blur the comparison between catatonia and non-catatonia groups.
PCS classification also depended on expert visual inspection. That is a reasonable method for a focused MRI morphology study, but it limits scale.
Future work would need automated or semi-automated sulcal-pattern tools before this could be tested in much larger datasets.
The practical takeaway is therefore narrow. The study does not show that an MRI fold can diagnose catatonia in the clinic.
It suggests that left anterior cingulate sulcal pattern may mark a developmental vulnerability associated with catatonia across psychiatric diagnoses.
That is still useful. Catatonia is often missed, even though treatments such as benzodiazepines and electroconvulsive therapy can be effective.
A stable vulnerability feature would not replace clinical recognition, but it could help researchers understand why catatonia clusters in some high-risk neurodevelopmental and psychiatric contexts.
Citation: DOI: 10.64898/2026.04.20.26351285. Moyal et al. Anterior Cingulate Cortex Sulcal Patterns associated with Catatonia across Schizophrenia and Mood Disorders. medRxiv. 2026.
Study Design: Retrospective hospital-based MRI morphology analysis of anterior cingulate sulcal patterns.
Sample Size: 523 participants: 109 patients with catatonia, 323 psychiatric patients without catatonia, and 91 healthy controls.
Key Statistic: Left PCS was present in 28% of catatonia patients versus 53% of psychiatric patients without catatonia; adjusted left-side group effect chi-square = 16.65, p = .0002.
Caveat: This was a preprint and retrospective MRI study, so the result needs prospective replication before clinical use.





