TL;DR: A 2026 study in BMC Psychiatry used Taiwan insurance records to find that dementia in people with schizophrenia was tied more strongly to age and linked medical comorbidities than to antipsychotic exposure after multivariable adjustment.
Key Findings
- 147 dementia cases: Researchers compared 147 people with schizophrenia who developed dementia with 882 sex- and diagnosis-year-matched schizophrenia controls.
- Age remained central: Dementia cases were older at the index date than controls, averaging 57.5 versus 40.5 years.
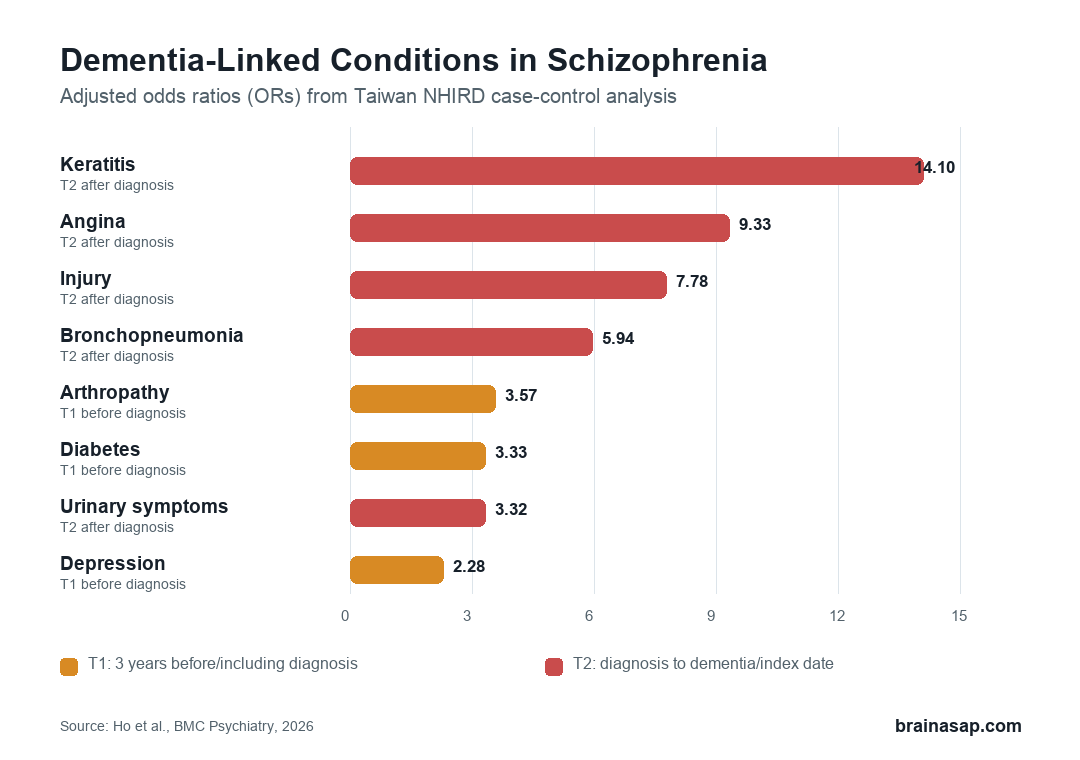
- Diabetes before diagnosis: Diabetes in the early interval was associated with higher dementia odds, with an adjusted odds ratio of 3.33.
- Later medical events stood out: Keratitis, angina, bronchopneumonia, urinary symptoms, injury, and related conditions showed elevated adjusted odds ratios in the later interval.
- Antipsychotic association weakened: Differences in antipsychotic use appeared in baseline comparisons, but antipsychotic associations did not persist after multivariable adjustment.
Source: BMC Psychiatry (2026) | Ho et al.
Schizophrenia is already linked to cognitive vulnerability, but the clinical question is more specific: when dementia appears later, is the risk mainly a medication story, a comorbidity story, or both?
This study used Taiwan’s National Health Insurance Research Database to examine that question over time. Researchers separated conditions that appeared around the schizophrenia diagnosis from conditions recorded later, then tested which factors still tracked dementia after adjustment.
Taiwan Claims Data Linked Schizophrenia, Dementia, and Comorbidities
The analysis started with a nationwide insurance database covering an 18-year observation period from 2000 to 2018. Cases were people with schizophrenia who later had dementia identified through diagnosis codes plus antidementia medication records.
Each dementia case was matched to six schizophrenia controls by sex and year of first schizophrenia diagnosis. That produced 147 dementia cases and 882 controls, giving the analysis a way to compare people with similar schizophrenia timing but different dementia outcomes.
The design used two time windows:
- T1 window: The 3 years before and including the schizophrenia diagnosis date.
- T2 window: The period from schizophrenia diagnosis to dementia diagnosis or the matched control index date.
- Valid diagnosis rule: A comorbidity had to appear in at least three outpatient visits or one inpatient admission.
This timing distinction reduces one common bias: early dementia symptoms can be mistaken for independent illnesses. The study also excluded dementia that appeared within 1 year of schizophrenia diagnosis.
Age Was a Major Dementia Risk Anchor
Age was the most obvious imbalance. The dementia group averaged 57.5 years at the index date, compared with 40.5 years in the control group.
The researchers did not age-match the groups because preliminary age matching reduced the sample too much. Instead, age stayed in the regression models as a covariate, which helps but does not erase the possibility of residual age confounding.
Some conditions linked with dementia in the models also become more common as people age. The associations are therefore not proof that each condition independently causes dementia.
Early Diabetes, Depression, Cataract, and Arthropathy Tracked Later Dementia
In the T1 period, the final adjusted model identified several conditions associated with later dementia risk in people with schizophrenia. These included diabetes, depressive disorder, cataract, menopausal or postmenopausal disorder, arthropathy, and age.
The strongest T1 estimates were not psychiatric medication measures. They were medical and psychiatric comorbidity markers:
- Arthropathy: Adjusted odds ratio 3.57, with 8.84% of dementia cases and 2.27% of controls having the diagnosis.
- Diabetes: Adjusted odds ratio 3.33, with 20.41% of dementia cases and 5.56% of controls in the T1 model table.
- Postmenopausal disorder: Adjusted odds ratio 2.70, with 10.88% of dementia cases and 1.70% of controls.
- Cataract: Adjusted odds ratio 2.52, with 11.56% of dementia cases and 1.36% of controls.
- Depressive disorder: Adjusted odds ratio 2.28, with 11.56% of dementia cases and 6.46% of controls.
These results do not mean cataract or joint disease directly causes dementia. They point to a broader clinical pattern: people with schizophrenia who later developed dementia carried more medical burden before or around the schizophrenia diagnosis.
Later Medical Events Formed a Comorbidity Network
The T2 model identified a different set of later conditions. Several had large adjusted odds ratios, including keratitis, angina, injury codes, bronchopneumonia, urinary-system symptoms, and organ or tissue replacement codes.
Path analysis then connected these conditions into a network. Early diabetes was linked with later urinary symptoms, angina, and organ replacement codes; early cataract was linked with later bronchopneumonia and organ replacement; early depression was linked with later shoulder or finger contusion.
The chart should be read as a cluster marker, not as a claim that every individual code is a screening target. In this dataset, multisystem health burden accumulated over time in the group that developed dementia.
Antipsychotic Differences Did Not Survive Adjustment
At baseline, antipsychotic use differed between groups. Atypical antipsychotic use was recorded in 77.55% of the dementia group and 69.50% of controls, and quetiapine use was 34.01% versus 16.89%.
Those raw differences are clinically relevant, but they were not the final answer. After multivariable adjustment, associations with antipsychotic use did not persist, while age and comorbidity patterns remained central.
The risk-direction issue is important:
- Medication exposure was not cleared as irrelevant: Claims data cannot measure illness severity, prescribing reasons, adherence, or cognitive testing.
- Medication was not the dominant adjusted finding: The final interpretation favored comorbidities and their timing over antipsychotic exposure alone.
- Clinical monitoring should stay broad: Cardiometabolic disease, injuries, infections, urinary symptoms, depression, and age-related medical burden may all matter in long-term care.
Claims Data Limits the Causal Claim
The study’s main strength is scale and longitudinal coverage. Taiwan’s insurance database gave researchers a large, structured record of diagnoses and prescriptions across years.
The main limitation is that insurance claims are not clinical examinations. The database lacked laboratory results, cognitive test scores, neuroimaging, education, smoking, alcohol use, diet, physical activity, and detailed schizophrenia severity.
Age matching was also not used, and the authors note that residual age confounding may remain. Depression and some other conditions could partly reflect prodromal dementia rather than independent risk factors, even with the study’s timing safeguards.
The clinical takeaway is therefore narrow and practical: in people with schizophrenia, dementia-risk monitoring should not focus only on antipsychotic exposure. This analysis supports closer attention to age, metabolic disease, depressive symptoms, injuries, infections, urinary symptoms, and broader medical complexity over time.
Citation: DOI: 10.1186/s12888-026-08072-3. Ho et al. Finding risk factors for dementia in patients with schizophrenia: a population-based case-control study. BMC Psychiatry. 2026.
Study Design: Nationwide population-based case-control study using Taiwan National Health Insurance Research Database records.
Sample Size: 147 schizophrenia patients with dementia and 882 matched schizophrenia controls.
Key Statistic: Six T1 and ten T2 factors were associated with dementia; T1 diabetes had an adjusted odds ratio of 3.33 and T2 keratitis had an adjusted odds ratio of 14.10.
Caveat: Claims data could not measure cognitive scores, disease severity, lifestyle factors, or medication adherence, and residual age confounding may remain.