TL;DR: A 2026 study in Annals of General Psychiatry found that, among 457 adults with recurrent major depressive disorder in Pakistan, escitalopram was the most common single antidepressant and reported side effects varied sharply by drug class.
Key Findings
- Clinic sample covered 457 adults: All participants had recurrent major depressive disorder and were recruited from psychiatry clinics in Lahore and Rawalpindi.
- Escitalopram led single-drug prescribing: Escitalopram was used by 12.9% of participants, while SSRIs as a class accounted for 32.1% of monotherapy prescriptions.
- Combination therapy was common: Two-antidepressant regimens were used by 26.7% of participants, most often mirtazapine plus escitalopram.
- Side effects clustered by class: TCAs had more nausea and vomiting, SNRIs had more urinary difficulty, and dual therapy showed more metabolic complaints.
- The Urdu checklist performed acceptably: The Urdu Antidepressant Side-Effect Checklist had a Cronbach’s alpha of 0.78, supporting its use as a patient-reported monitoring tool.
Source: Annals of General Psychiatry (2026) | Riaz et al.
Antidepressant side effects are often treated as a secondary issue, but they can decide whether depression care actually continues. In this cross-sectional study, researchers used prescribing records and patient-reported symptoms to map how different antidepressant regimens looked in two Pakistani psychiatry clinics.
The focus was adults with major depressive disorder (MDD), a clinical diagnosis of depression. Every participant in the sample had recurrent MDD, meaning the illness was not a first episode.
SSRIs Dominated Single-Drug Antidepressant Prescribing
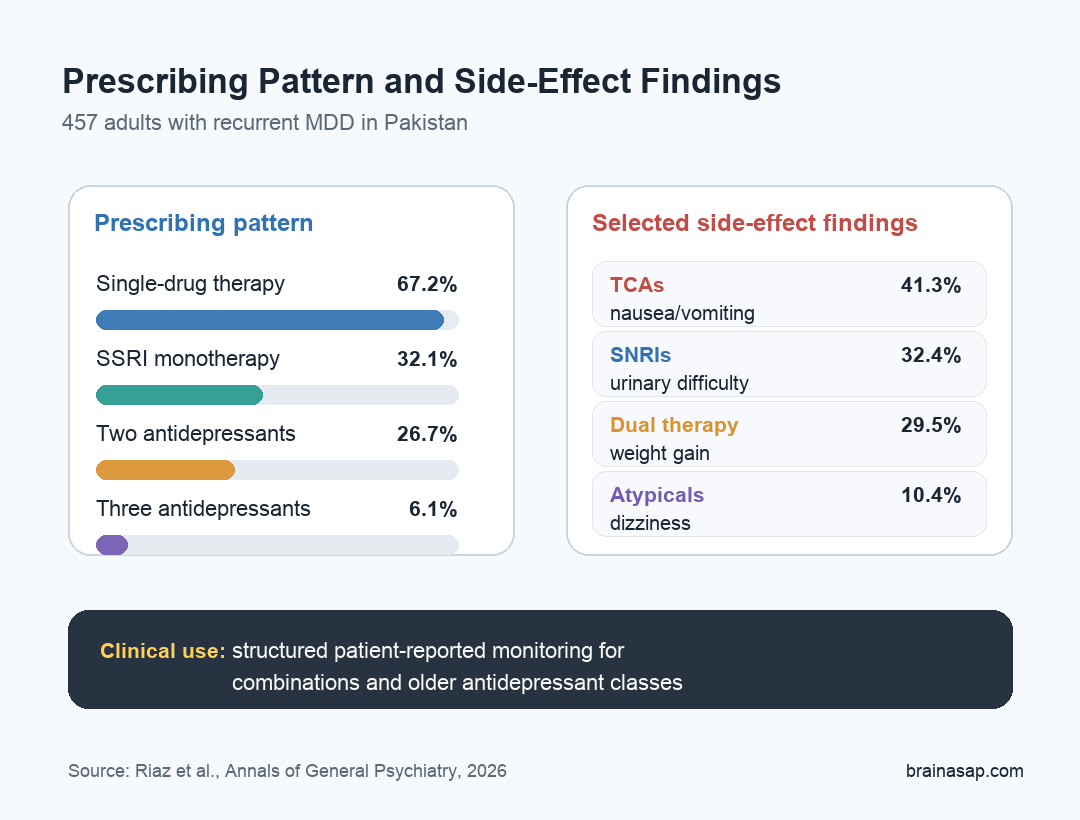
The clearest prescribing pattern was the reliance on single-drug therapy. Of the 457 participants, 307 people, or 67.2%, were treated with one antidepressant rather than a combination.
Selective serotonin reuptake inhibitors, or SSRIs, were the largest single-drug class. SSRIs are antidepressants that primarily increase serotonin signaling by reducing serotonin reuptake. In this sample, they accounted for 32.1% of monotherapy prescriptions.
The main single-drug options broke down this way:
- Escitalopram: 59 participants, or 12.9% of the total sample.
- Paroxetine: 28 participants, or 6.1%.
- Fluoxetine and sertraline: 27 participants each, or 5.9% for each drug.
- Fluvoxamine: 6 participants, or 1.3%.
The SSRI-heavy pattern fits the broader clinical preference for SSRIs as first-line antidepressants, but the study adds local detail from Pakistan rather than importing assumptions from high-income health systems.
Combination Therapy Was Not Rare in Recurrent MDD
Combination therapy also mattered. Researchers reported that 122 participants, or 26.7%, were taking two antidepressants, and another 27 participants, or 6.1%, were taking three-drug regimens.
The most common two-drug pair was mirtazapine plus escitalopram, used by 56 participants. Mirtazapine plus fluoxetine was next, used by 25 participants.
The three-drug regimens were less frequent but clinically important because they increase monitoring complexity. Fluoxetine plus duloxetine plus clomipramine appeared in 18 participants, while duloxetine plus amitriptyline plus agomelatine appeared in 9.
Patient-Reported Side Effects Differed by Drug Class
The study used the Urdu Antidepressant Side-Effect Checklist, or U-ASEC, a translated patient-reported checklist for antidepressant adverse effects. Its internal consistency was acceptable, with Cronbach’s alpha = 0.78.
Factor analysis grouped symptoms into three broad clusters:
- Autonomic symptoms: body-system effects such as dry mouth, urination problems, and orthostatic symptoms.
- Central nervous system symptoms: effects such as dizziness, tremor, or spinning-room sensations.
- Metabolic symptoms: effects such as weight gain and increased body temperature.
Dry mouth and insomnia were the most frequently reported side effects among SSRI users. Tricyclic antidepressants, or TCAs, had higher nausea and vomiting rates, reported at 41.3%.
Serotonin-norepinephrine reuptake inhibitors, or SNRIs, were associated with more urinary difficulty, reported at 32.4%. Atypical antidepressants showed a mixed profile: lower dry mouth, reported at 18.8%, but higher dizziness, reported at 10.4%.
Regression Results Pointed to Specific Monitoring Targets
The multivariable models adjusted for age, sex, tobacco use, comorbidity, and duration of MDD. A raw side-effect percentage can reflect who received the drug, not only the drug itself.
After adjustment, several class-specific associations remained:
- TCAs and nausea: TCAs were linked to higher odds of nausea, with an odds ratio of 3.96.
- TCAs and urinary problems: TCAs were also linked to higher odds of urination problems, with an odds ratio of 2.77.
- SNRIs and urinary difficulty: SNRIs had a higher odds estimate for urinary difficulty, with an odds ratio of 12.92, though the confidence interval was wide.
- Atypicals and dizziness: Atypical antidepressants were linked to higher dizziness odds, with an odds ratio of 8.42.
These estimates should not be read as a treatment ranking. They are monitoring signals from an observational clinic sample, not randomized drug comparisons.
The Main Clinical Use Is Better Side-Effect Monitoring
The strongest practical point is not that one antidepressant class should replace another. It is that side-effect monitoring needs to be structured, especially when patients are taking combinations or older antidepressant classes.
A translated checklist can help clinicians ask about symptoms that patients may not volunteer. That is especially relevant in settings where time, stigma, and medication access can make follow-up uneven.
Three caveats keep the result bounded:
- Cross-sectional design: The data capture prescribing and symptoms at one point, so causality cannot be proven.
- Convenience sampling: Participants came from two clinics, which may not represent all depression care in Pakistan.
- Self-reported symptoms: Patient reports are clinically valuable but still depend on recall and interpretation.
Even with those limits, the study gives clinicians a concrete map: which antidepressant patterns were common, which symptom clusters appeared, and where routine monitoring may need to be more deliberate.
Citation: DOI: 10.1186/s12991-026-00644-7. Riaz et al. Antidepressant prescribing patterns and patient-reported adverse effects: a cross-sectional study from Pakistan. Annals of General Psychiatry. 2026.
Study Design: Cross-sectional questionnaire-based study at two psychiatry clinics in Lahore and Rawalpindi.
Sample Size: 457 adults with recurrent major depressive disorder.
Key Statistic: Escitalopram was the most common single agent at 12.9%; SSRIs made up 32.1% of monotherapy prescriptions, and two-antidepressant therapy was used by 26.7%.
Caveat: Observational clinic sample with convenience recruitment, so prescribing patterns and side-effect associations may not generalize to all patients with depression.