TL;DR: A 2026 narrative review in the Japanese Journal of Radiology reported that Alzheimer’s brain positron emission tomography (PET) imaging has shifted from supportive diagnosis toward treatment selection because amyloid PET is now central to confirming eligibility for anti-amyloid antibody therapy.
Key Findings
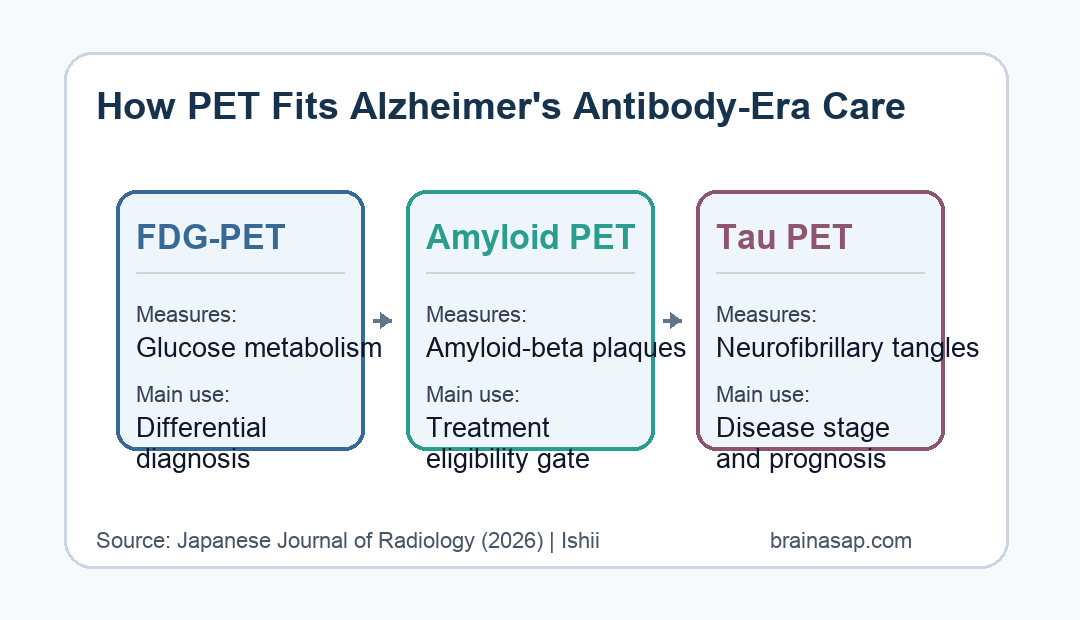
- Three PET roles: The review separated FDG-PET, amyloid PET, and tau PET by what each scan measures in Alzheimer’s disease.
- Amyloid eligibility gate: Amyloid PET can visualize cerebral amyloid-beta deposition and is used to confirm amyloid positivity before anti-amyloid antibody treatment.
- Negative amyloid scan: A negative amyloid PET scan makes Alzheimer’s disease unlikely as the primary cause of cognitive impairment in the review’s clinical framing.
- Quantitative standards: Standardized uptake value ratios and the Centiloid scale were highlighted as tools for comparing amyloid PET results across sites.
- Tau staging role: Tau PET was described as a complementary marker for neurofibrillary pathology, disease severity, progression, and patient stratification.
Source: Japanese Journal of Radiology (2026) | Ishii
Brain positron emission tomography (PET) is becoming more practical in Alzheimer’s care because treatment decisions increasingly depend on whether the disease biology is present, not only whether symptoms fit a dementia syndrome.
The review’s main message is that PET scans answer different questions. Glucose metabolism, amyloid plaques, and tau tangles are related to Alzheimer’s disease, but they are not interchangeable signals.
Amyloid PET Now Helps Decide Alzheimer’s Treatment Eligibility
Anti-amyloid-beta antibodies such as lecanemab and donanemab changed the clinical role of biomarker testing. If a treatment is meant to remove or reduce amyloid pathology, the patient first needs evidence that amyloid is actually present.
In this review, amyloid PET is the central imaging test for that question. It allows noninvasive visualization of cerebral amyloid-beta deposition, making it useful when clinicians are considering disease-modifying therapy in mild cognitive impairment or mild dementia.
- Positive amyloid scan: Supports that amyloid pathology is present and may fit the biological entry requirement for anti-amyloid treatment.
- Negative amyloid scan: Argues against Alzheimer’s disease as the main driver of cognitive impairment, even when symptoms look concerning.
- Appropriate-use boundary: The review emphasizes use in symptomatic patients where the result can change treatment decisions, not broad screening of healthy people.
That distinction has direct clinical value because Alzheimer’s symptoms can overlap with other neurodegenerative dementias, vascular disease, psychiatric conditions, medication effects, and normal aging. A scan that clarifies the underlying protein pathology can change what happens next.
FDG-PET Supports Dementia Differential Diagnosis
FDG-PET measures cerebral glucose metabolism, a proxy for regional neuronal and synaptic activity. The review describes it as useful for recognizing characteristic hypometabolic patterns in Alzheimer’s disease, dementia with Lewy bodies, and frontotemporal lobar degeneration.
FDG-PET is therefore still clinically valuable, but it is not the same kind of test as amyloid PET. It can show where the brain is underactive; it does not directly show amyloid plaques or tau tangles.
- Alzheimer’s pattern: FDG-PET can support a diagnosis when the metabolic pattern fits Alzheimer’s disease.
- Lewy body and FTD patterns: Different hypometabolic patterns can help separate other neurodegenerative dementias.
- Supportive role: Because FDG-PET does not visualize molecular pathology, it remains supportive rather than definitive for antibody-treatment eligibility.
The review also notes a policy difference. FDG-PET has been covered in the United States for distinguishing Alzheimer’s disease from frontotemporal dementia since 2004, while Japan has not reimbursed it for dementia differential diagnosis.
Centiloid Scaling Makes Amyloid PET Easier to Compare
Visual interpretation remains important, but the review highlights quantitative approaches because Alzheimer’s imaging is moving into routine treatment pathways. Standardized uptake value ratios compare tracer uptake in target brain regions with a reference region.
The Centiloid scale is a second standardization tool. It helps place amyloid PET results onto a common scale so findings are more comparable across tracers, scanners, institutions, and research studies.
- Tracer differences: The review discusses 18F-labeled amyloid tracers such as florbetapir, flutemetamol, and florbetaben.
- Reading standards: Tracer-specific acquisition and interpretation guidelines reduce the chance that similar scans are read inconsistently.
- Workflow pressure: As anti-amyloid treatment expands, clinics need reproducible imaging pathways rather than one-off expert readings.
This is not only a technical issue. Treatment eligibility, counseling, and monitoring can all be affected if one site calls a scan positive while another site would treat the same biology as borderline.
Tau PET Adds Disease Stage and Prognosis Context
Tau PET visualizes neurofibrillary pathology rather than amyloid plaque burden. That gives it a different clinical role: it can help describe disease stage, severity, and likely progression.
The review frames tau PET as complementary to amyloid PET. Amyloid positivity may be needed to enter an anti-amyloid treatment pathway, while tau burden can help explain how far the disease process has advanced.
- Pathology target: Tau PET reflects neurofibrillary tangles, a core Alzheimer’s pathology linked with clinical severity.
- Patient stratification: Tau information may help classify patients by disease stage or progression risk.
- Complementary use: Tau PET does not replace amyloid confirmation when the treatment question is amyloid-targeted therapy.
For patients and clinicians, that means one scan type may answer “is the amyloid target present?” while another helps answer “how advanced does the Alzheimer’s process look?”
AI and Dedicated Brain PET Could Improve Dementia Imaging Workflows
The review closes by pointing to two practical directions: high-resolution dedicated brain PET systems and artificial intelligence-based image analysis. Both could make dementia imaging clearer and easier to use at scale.
Dedicated brain PET systems may improve spatial resolution for smaller brain structures. AI tools may help with image analysis, quality control, quantification, and workflow efficiency.
- Diagnostic performance: Better hardware could improve visualization of regional uptake patterns.
- Efficiency: AI-assisted analysis may reduce manual workload in busy dementia imaging programs.
- Caveat: The review is a narrative synthesis, not a trial showing that AI-driven PET workflows improve patient outcomes.
The practical takeaway is measured. PET is not a standalone dementia answer, but in the anti-amyloid era it is becoming part of the evidence chain that links symptoms, molecular pathology, treatment eligibility, and prognosis.
Citation: DOI: 10.1007/s11604-026-01998-4. Ishii. Brain PET in the era of anti-amyloid-beta antibody therapy for Alzheimer disease. Japanese Journal of Radiology. 2026.
Study Design: Narrative review of FDG-PET, amyloid PET, tau PET, clinical guidelines, and methodological issues in Alzheimer’s disease imaging.
Sample/Model: Literature-based review focused on Alzheimer’s disease diagnosis, biomarker confirmation, treatment eligibility, and disease monitoring.
Key Statistic: Amyloid PET is described as indispensable for anti-amyloid antibody eligibility, while FDG-PET remains supportive because it does not directly measure molecular pathology.
Caveat: The review summarizes imaging roles and guidelines rather than testing a new PET strategy in a patient cohort.