TL;DR: A 2026 study protocol in Trials describes COSTS, a randomized trial that will compare cognitive behavioral therapy for insomnia (CBT-I) with standard cognitive behavioral therapy (CBT) in 60 people with treatment-resistant schizophrenia and persistent sleep disturbance.
Key Findings
- Planned sample: Researchers aim to enroll 60 adults with treatment-resistant schizophrenia or related chronic psychosis plus insomnia symptoms lasting at least 3 months.
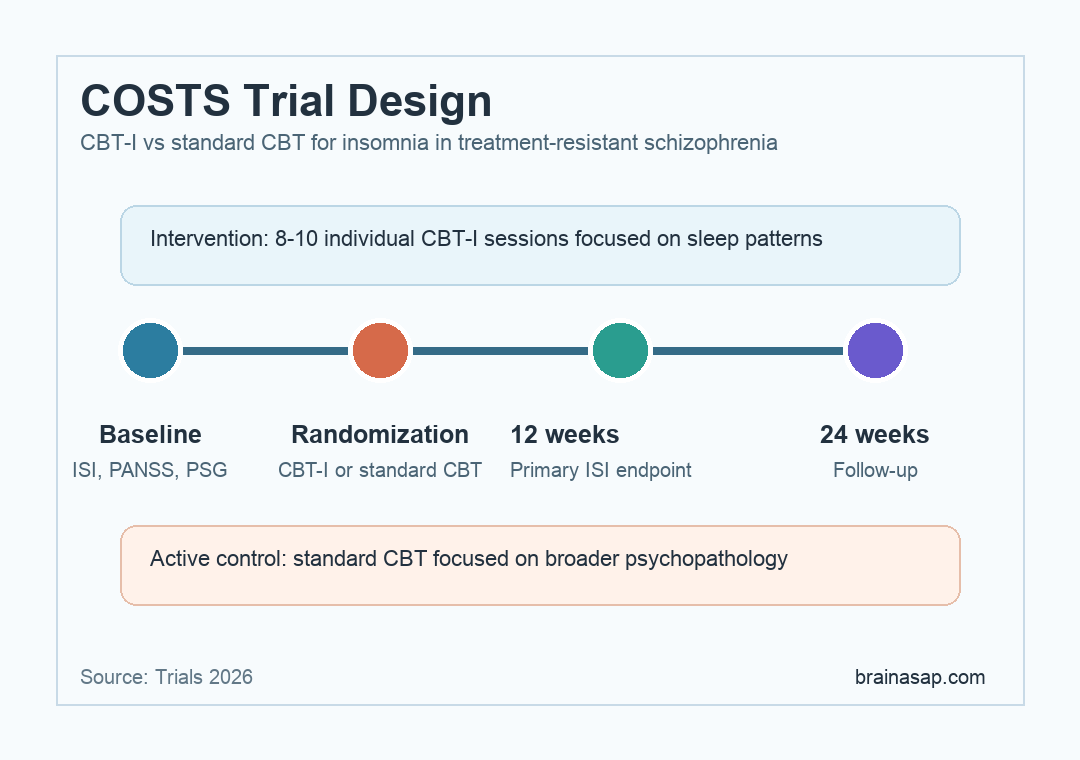
- Trial comparison: Participants will be randomized to 8-10 individual sessions of CBT-I or standard CBT over about 12 weeks.
- Primary outcome: The main endpoint is change in the Insomnia Severity Index (ISI), a self-report insomnia scale, after 12 weeks.
- Follow-up plan: Assessments occur at baseline, 12 weeks, and 24 weeks, with polysomnography included at baseline and 12 weeks.
- Main boundary: This is a study protocol, so it explains the planned test but does not report whether CBT-I works in this group.
Source: Trials (2026) | Johansen et al.
Treatment-resistant schizophrenia creates a difficult clinical problem: antipsychotic medication does not sufficiently reduce symptoms for a substantial subgroup, and sleep disturbance can add another layer of impairment.
In this setting, insomnia is not just a comfort issue. Poor sleep can worsen anxiety, daytime function, and the strain of managing persistent psychotic symptoms.
The planned trial is not testing a new drug. It is testing whether CBT-I, a structured insomnia treatment, adds a more targeted sleep pathway for patients whose psychosis has remained clinically difficult despite pharmacological care.
CBT-I Will Be Compared With Standard CBT in 60 Patients
Researchers plan to enroll 60 patients from a specialized complex-schizophrenia outpatient clinic in Copenhagen. Eligible patients can have schizophrenia, chronic paranoid psychosis, schizoaffective psychosis, or another non-organic chronic psychosis with a history of treatment resistance.
Sleep disturbance is not a loose complaint in the protocol. Participants must have sleeping difficulties for at least 3 months and an ISI score of 15 or higher, which places insomnia symptoms in the clinically relevant range.
- Diagnosis: Schizophrenia or a related chronic psychosis diagnosis.
- Psychosis severity: Ongoing positive symptoms despite adequate antipsychotic treatment.
- Sleep threshold: Persistent sleep disturbance plus an ISI score of at least 15.
- Medication stability: Stable pharmacological treatment for at least 1 month.
The age range is 18-64 years. The protocol excludes people whose recent hospitalization, substance use, or sleep apnea treated with continuous positive airway pressure (CPAP) could make the intervention harder to interpret.
The Intervention Targets Insomnia Rather Than Psychosis Alone
Both groups will receive individual psychotherapy, but the treatment targets differ. The active intervention is CBT-I, which focuses on sleep patterns, sleep-related beliefs, bedtime behaviors, and daytime activity.
The active control is standard CBT, focused on broader psychopathology rather than a dedicated insomnia protocol.
The sleep focus is clinically relevant because sleep disturbance and psychotic symptoms can reinforce each other. Insomnia can worsen anxiety, rumination, and paranoia, while psychotic symptoms can disrupt sleep routines and increase nighttime arousal.
- CBT-I group: Receives sleep-focused cognitive and behavioral treatment over 8-10 sessions.
- Standard CBT group: Receives individual CBT focused on psychopathology rather than a dedicated insomnia protocol.
- Therapy window: Sessions take place over roughly 12 weeks.
The protocol’s central hypothesis is straightforward: both groups may improve, but CBT-I should produce larger sleep improvements because it directly targets insomnia mechanisms.
ISI at 12 Weeks Is the Primary Sleep Endpoint
The primary outcome is improvement on the Insomnia Severity Index after 12 weeks. ISI is a rating scale that captures perceived insomnia severity, sleep satisfaction, functional interference, and distress from sleep problems.
Secondary outcomes broaden the picture beyond insomnia. Researchers will assess psychotic symptoms, functioning, recovery, well-being, treatment expectations, and objective sleep architecture.
- Psychosis symptoms: Positive and Negative Syndrome Scale (PANSS), a clinician-rated schizophrenia-symptom scale.
- Functioning: Global Assessment of Functioning, Functional Assessment Short Test, and Personal and Social Performance Scale.
- Well-being and recovery: WHO-5 well-being score and Process of Recovery Questionnaire.
- Objective sleep: Polysomnography measures such as sleep latency, wake after sleep onset, sleep efficiency, and total sleep time.
Polysomnography is included at baseline and 12 weeks, but not at the 24-week follow-up. That design lets researchers compare subjective insomnia change with objective sleep physiology during the main treatment period.
The Protocol Is Powered for a 4-Point ISI Difference
The sample-size plan is based on detecting a 4-point between-group difference on ISI with 80% power. Researchers estimate that follow-up data from 24 patients per group are needed, then raise total enrollment to 60 to allow for about 25% attrition.
This is the central statistical boundary: the study is designed around a clinically interpretable insomnia change, not around proving broad recovery from schizophrenia.
- Primary endpoint: CBT-I is expected to improve insomnia more than standard CBT after 12 weeks.
- Secondary symptom link: Sleep improvements will be compared with changes in positive symptoms and functioning.
- Objective sleep measure: Sleep-lab measures will be compared with self-reported insomnia change.
The authors also expect that improved sleep may correlate with improved positive symptoms. That would not by itself prove causality, but it would support the idea that sleep treatment can matter in complex psychosis care.
COSTS Defines CBT-I Endpoints Before Efficacy Data Arrive
COSTS is useful because it separates two psychotherapy pathways that are often blurred. Standard CBT can address psychosis-related distress, while CBT-I tests a narrower sleep mechanism that might be easier to implement if the trial is positive.
The protocol also keeps measurement practical. It combines self-report, clinician-rated symptoms, functioning scales, and sleep-lab data, which reduces the risk that one scale will carry the whole interpretation.
Clinical boundary: readers should not treat this protocol as evidence that CBT-I already improves sleep or psychosis in treatment-resistant schizophrenia.
The planned trial defines the patient group, intervention dose, primary endpoint, and follow-up schedule clearly enough for the results to be interpretable when they arrive.
Citation: DOI: 10.1186/s13063-026-09482-0. Johansen et al. Cognitive behavioral therapy for insomnia vs. standard cognitive behavioral therapy for sleep and circadian disturbances in treatment-resistant schizophrenia: study protocol for the randomized controlled trial (COSTS). Trials. 2026;27:309.
Study Design: Randomized controlled trial protocol comparing CBT-I with standard CBT.
Sample Size: Planned enrollment of 60 adults with treatment-resistant schizophrenia or related chronic psychosis and persistent sleep disturbance.
Key Statistic: The trial is powered to detect a 4-point between-group difference on the Insomnia Severity Index at 12 weeks.
Caveat: The paper reports a protocol, so treatment efficacy results are not yet available.