TL;DR: A 2026 study in Neuropsychopharmacology Reports found that repeated cigarette smoking and quitting shifted clozapine metabolism in one Japanese man with treatment-resistant schizophrenia, with the dose-adjusted clozapine level falling during smoking periods.
Key Findings
- One patient was followed across five periods: Researchers tracked a Japanese man in his 40s across smoking, quitting, smoking, quitting, and resumed-smoking periods while he was taking clozapine.
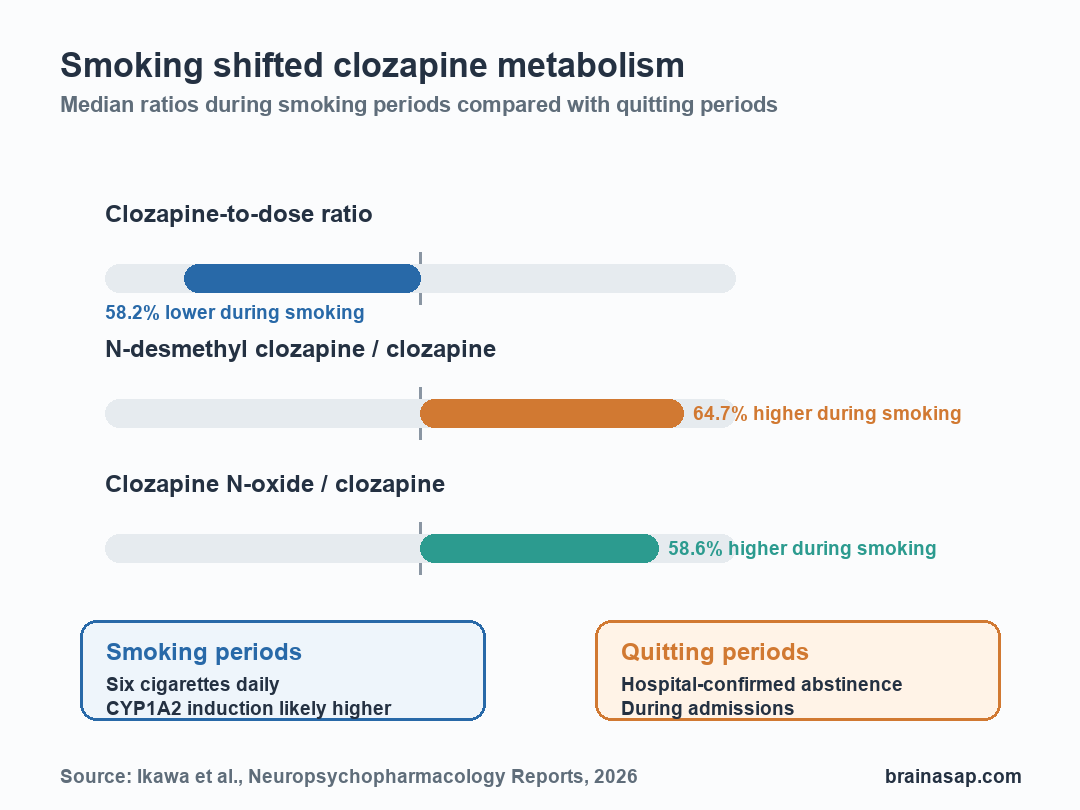
- Smoking lowered the clozapine dose ratio: The clozapine-to-dose ratio was 58.2% lower during smoking periods than during quitting periods.
- Metabolite ratios moved the other way: The N-desmethyl clozapine/clozapine ratio was 64.7% higher during smoking, and the clozapine N-oxide/clozapine ratio was 58.6% higher.
- CYP1A2 is the practical mechanism: Cigarette smoke can induce cytochrome P450 1A2 (CYP1A2), a liver enzyme involved in clozapine metabolism, even when the reported smoking level is modest.
- The evidence remains narrow: This was a single-patient case report, so it supports careful monitoring rather than a universal dose rule.
Source: Ikawa et al. reported repeated smoking and quitting periods during clozapine treatment in a patient with schizophrenia.
Smoking Status Was the Variable Clinicians Could Miss
Clozapine is one of the most important drugs for treatment-resistant schizophrenia, but it has a narrow clinical-management window. Blood levels matter because too little exposure can weaken symptom control, while too much exposure can raise safety concerns.
This case report focused on a common real-world problem: smoking status changes. Patients with schizophrenia smoke at higher rates than the general population, and some quit during hospitalization only to resume smoking after discharge.
Cigarette smoke affects drug metabolism through a clinically relevant pathway. The key pathway here is CYP1A2, a liver enzyme that helps metabolize clozapine.
When smoking induces CYP1A2 activity, clozapine can be cleared faster.
The patient in this report had an on-off pattern that complicates medication management:
- Period I: Smoking during weeks 1-79.
- Period II: Quitting during weeks 80-84 while hospitalized.
- Period III: Smoking again during weeks 85-140.
- Period IV: Quitting again during weeks 141-148 while hospitalized.
- Period V: Smoking again after discharge.
Dose-Adjusted Clozapine Was Lower During Smoking
Researchers measured trough plasma concentrations, meaning blood was drawn before the next clozapine dose, about 10-14 hours after the previous dose. They measured unchanged clozapine, N-desmethyl clozapine, and clozapine N-oxide.
The cleanest number was the clozapine-to-dose ratio, abbreviated CLZ/D. This ratio helps separate blood exposure from the prescribed daily dose, which ranged from 300 to 425 mg/day in the report.
During the combined smoking periods, the median CLZ/D ratio was 0.3485. During the combined quitting periods, it was 0.834. The difference translated to a 58.2% lower dose-adjusted clozapine level during smoking.
The patient was not described as a heavy smoker. He reported six cigarettes daily during outpatient periods.
The authors noted that prior research suggests the smoking effect on clozapine can approach a near-maximal range at relatively low cigarette counts.
Metabolite Ratios Pointed Toward Faster Metabolism
The metabolite ratios moved in the opposite direction. During smoking periods, the N-desmethyl clozapine/clozapine ratio was 64.7% higher than during quitting periods. The clozapine N-oxide/clozapine ratio was 58.6% higher.
Those ratios matter because they help interpret whether clozapine is being metabolized differently rather than simply taken inconsistently. The authors emphasized that unchanged clozapine and both major metabolites shifted with smoking status.
The findings fit a straightforward pharmacology explanation:
- When smoking resumed: CYP1A2 activity likely increased, pushing more clozapine toward metabolism and lowering the dose-adjusted clozapine level.
- When smoking stopped: CYP1A2 induction likely faded, allowing clozapine exposure to rise relative to dose.
- When smoking resumed again: The same direction of change appeared again, making the effect look reproducible in this patient.
The report adds a metabolite detail beyond many smoking-clozapine discussions: clozapine N-oxide was followed over time, not only unchanged clozapine or N-desmethyl clozapine.
Hospitalization Can Hide the Smoking Change
The clinical risk is not only that a patient smokes. Smoking status can change at exactly the moments when care setting changes.
In this report, quitting periods nearly overlapped with hospitalization, while smoking resumed after discharge.
This creates two practical problems. A stable outpatient dose may become too high after abrupt smoking cessation.
A dose that looked adequate during a smoke-free hospitalization may become too low when the patient resumes cigarettes at home.
For clozapine management, the study points to a simple monitoring checklist:
- Ask directly about smoking changes: Current cigarette use is clinically relevant, not just background history.
- Check clozapine concentration: Blood levels can clarify whether exposure shifted after smoking cessation or resumption.
- Review dose after transitions: Hospital admission, discharge, smoking bans, quit attempts, and relapse to smoking all deserve medication review.
- Interpret metabolite ratios carefully: N-desmethyl clozapine/clozapine and clozapine N-oxide/clozapine ratios may help separate metabolism, adherence, and illness-related changes.
The Case Does Not Create a Universal Dose Rule
This was a single-patient case report. The quitting periods had only two sampling points each, and hospitalization itself could have changed adherence, nutrition, sleep, or other clinical factors.
The report also did not use detailed symptom-rating scales to map blood concentration changes onto clinical response. The strongest claim is pharmacokinetic, not a symptom-change claim after each smoking transition.
Still, the case is clinically useful because the direction of the signal was consistent with known clozapine metabolism. Smoking periods repeatedly aligned with lower dose-adjusted clozapine and higher metabolite ratios; quitting periods aligned with higher clozapine exposure.
The practical conclusion is narrow and important: in clozapine-treated schizophrenia, smoking status is not a minor lifestyle variable. It can change the drug exposure clinicians are trying to manage.
Citation: DOI: 10.1002/npr2.70121. Ikawa et al. Effects of Repeated Smoking and Quitting Cigarettes on Plasma Concentrations of Clozapine and Its N-Desmethyl and N-Oxide Metabolites in a Japanese Patient With Schizophrenia. Neuropsychopharmacology Reports. 2026;46:e70121.
Study Design: Single-patient pharmacokinetic case report across repeated smoking and quitting periods.
Sample Size: One Japanese man in his 40s with treatment-resistant schizophrenia.
Key Statistic: The median clozapine-to-dose ratio was 58.2% lower during smoking periods than during quitting periods.
Caveat: Sampling was limited, quitting periods overlapped with hospitalization, and the case cannot define a general clozapine dose adjustment rule.