TL;DR: A 2026 descriptive study in JMIR Formative Research reported that the NYUCI-ES dementia-caregiver program required 24 documented cultural adaptations before and during delivery to Chinese and Korean American caregivers.
Key Findings
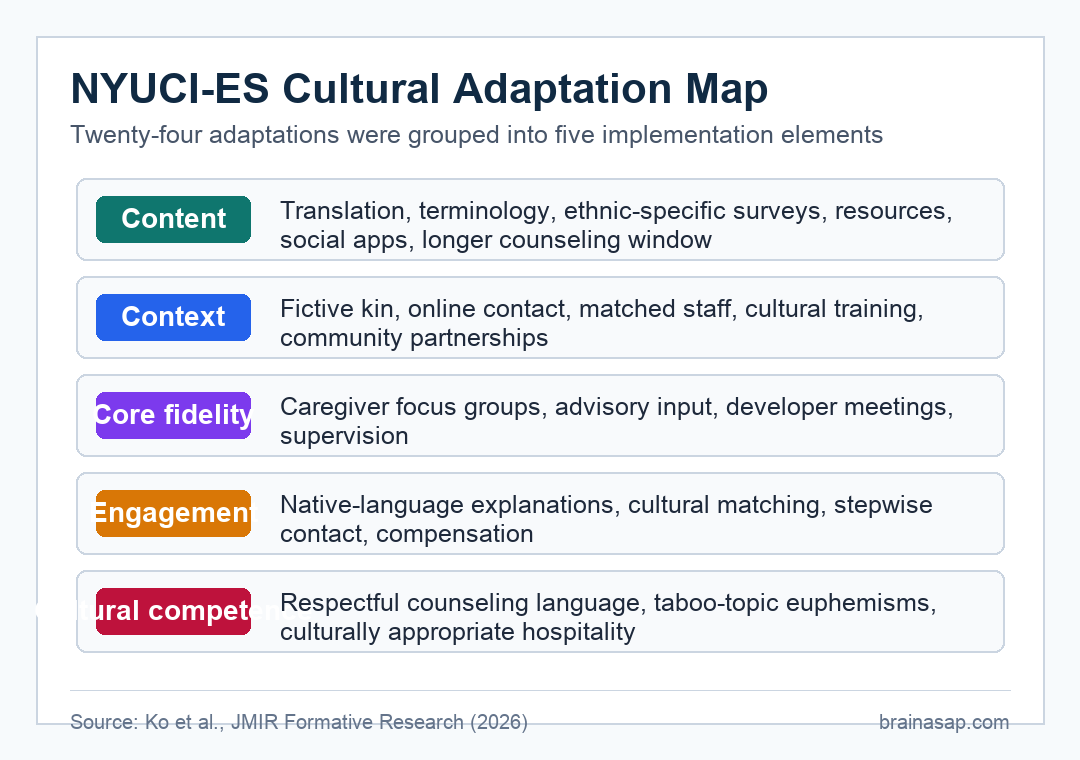
- 24 adaptation strategies: Researchers identified 24 major changes to the dementia-caregiver intervention.
- Five adaptation elements: Changes were grouped into content, context, relationship fidelity, engagement, and cultural competence.
- Six counseling sessions: The intervention kept six counseling sessions but extended the completion window to better fit family availability.
- Three assessment visits: The parent trial included baseline, 6-month, and 12-month assessment visits.
- Two adaptation frameworks: The team combined Day et al.’s cultural-adaptation elements with the FRAME system for timing and response type.
Source: JMIR Formative Research (2026) | Ko et al.
NYUCI-ES is a culturally adapted version of the New York University Caregiver Intervention for Chinese and Korean American dementia caregivers. Instead of testing whether the program improved caregiver health, this report documented what had to change so the intervention could fit the target communities.
Dementia-caregiver support often fails when a program assumes one family structure, one language environment, or one model of counseling.
Ko et al. treated adaptation as an implementation task, not as a cosmetic translation step.
NYUCI-ES Adapted Dementia Caregiver Counseling Across Five Domains
The study used deductive content analysis, a method that organizes observed material under an existing framework. Two team members first coded the adaptation strategies, then additional members reviewed and refined the categories.
The final map placed the changes into five domains. Each domain addressed a different way that a caregiver intervention can miss its intended audience if the original format is copied too literally.
- Content: Materials were translated, terminology was adjusted, ethnic-specific surveys and resources were added, and social media support was moved onto platforms already used by Chinese and Korean participants.
- Context: Family counseling eligibility expanded to include fictive kin, and communication shifted toward online and app-based contact when that matched participant habits.
- Relationship fidelity: The team consulted community experts, held caregiver focus groups, met regularly with the original program developer, and maintained counseling supervision.
- Engagement: Procedures and benefits were explained in participants’ native languages, staff roles were clarified, contact was prolonged, and compensation was used to support participation.
- Cultural competence: Counseling techniques were adjusted for cultural beliefs, taboo topics were handled with more careful language, and refreshments were used as a respectful relationship-building practice.
This structure kept the intervention recognizable while changing how it met families. The adaptation produced a more population-specific delivery system for Chinese and Korean American dementia caregiving, not a new counseling theory.
Translation Was Only One Part of Cultural Adaptation
Language access was important, but it was not the full adaptation. The program also had to adjust family roles, technology choices, communication style, counseling pacing, and trust-building.
The content changes included translated materials and multilingual support. They also included culturally relevant terminology and images, plus additional survey content on familism, stigma, and social support.
- Program materials: Translation helped participants understand study procedures and counseling content in English, Chinese, or Korean.
- Family meaning: Familism and social support were measured because caregiving decisions may involve relatives beyond a single primary caregiver.
- Communication platforms: Social media support groups used apps that participants already used, reducing the burden of learning a new channel.
The counseling schedule also changed. NYUCI-ES retained the six-session counseling structure, but the completion period expanded to 4 to 6 months because family-based sessions can be hard to schedule across households and work routines.
Family Counseling Expanded Beyond the Nuclear Family
One of the more concrete context changes was the inclusion of fictive kin, meaning close nonbiological relationships that function like family. That choice is practical for dementia caregiving because real caregiving networks do not always match narrow eligibility rules.
The intervention also used culturally matched staff and training on Korean and Chinese caregiving contexts. Those changes were meant to improve trust and reduce the chance that counseling would feel unfamiliar, intrusive, or culturally mismatched.
- Eligibility change: Family counseling could include people who mattered to the caregiving arrangement, not only conventional relatives.
- Personnel change: Participants were matched with social workers who shared cultural backgrounds when possible.
- Community partnership: Recruitment and delivery relied on culturally tailored organizations and outreach settings.
The parent trial enrolled Chinese or Korean Americans aged 50 years or older in the New York metropolitan area who cared for someone with memory problems and had at least one cardiometabolic risk factor.
This population detail is important because the adaptation was built around a specific caregiver-health trial, not a generic dementia education campaign.
Real-Time Feedback Changed Implementation During the Study
The team separated proactive changes made during preparation from reactive changes made during implementation. That timing distinction is useful because not every cultural barrier is visible before participants start using the program.
For example, the team planned multilingual materials and cultural matching in advance. Other changes, such as prolonged communication and relationship-building adjustments, emerged as staff learned what participants needed to feel comfortable with counseling.
- Preparation-stage adaptations: Translation, cultural training, study-procedure explanation, and community-board input could be planned before intervention delivery.
- Implementation-stage adaptations: Contact strategy, rapport-building, and some family-session adjustments developed after real participant interaction.
- Fidelity safeguard: Regular meetings with the original intervention developer helped keep the active ingredients of NYUCI while changing delivery details.
This is the main implementation lesson. A culturally adapted caregiver program needs both a plan and a feedback loop, especially when counseling is less familiar or more stigmatized in the target community.
The Report Documents Implementation, Not Caregiver Outcomes
The clearest limitation is that this publication does not report whether NYUCI-ES improved caregiver burden, mental health, cardiometabolic markers, or care-recipient outcomes. It describes how the adaptation was done.
The study is useful for program builders but limited for clinical decision-making. A reader should not treat the 24 adaptations as proof that the intervention works; they are a structured description of how researchers prepared the intervention for a specific population.
- Strength: The adaptation process was documented with established frameworks instead of informal notes.
- Boundary: The report focuses on Chinese and Korean American caregivers in one metropolitan trial context.
- Next evidence need: Outcome data from the ongoing trial will be needed to test whether the adapted intervention improves caregiver health.
For dementia-caregiver research, the implementation point is narrow: cultural fit has to be designed at the level of language, family roles, staff relationships, technology, timing, and counseling norms.
Citation: DOI: 10.2196/86499. Ko et al. Exploring the Cultural Adaptation of an Ongoing Evidence-Based Intervention for Chinese and Korean American Dementia Caregivers: Descriptive Study. JMIR Formative Research. 2026;10:e86499.
Study Design: Descriptive implementation study using deductive content analysis of cultural adaptation strategies.
Sample/Model: NYUCI-ES, an ongoing caregiver intervention trial for Chinese and Korean American dementia caregivers in the New York metropolitan area.
Key Statistic: Researchers identified 24 major adaptation strategies across five cultural-adaptation elements.
Caveat: The report documents adaptation methods, not the intervention’s clinical effectiveness.