TL;DR: A 2026 systematic review and meta-analysis in Lupus found that psychosis affected about 4.5% of adults with systemic lupus erythematosus (SLE), was more common in neuropsychiatric SLE, and tracked most strongly with active immune disease markers rather than serving as a stand-alone psychiatric label.
Key Findings
- Sixty-five studies were included: The review covered 31,495 adults with systemic lupus erythematosus across cohort, cross-sectional, case-control, and mixed designs.
- Pooled SLE psychosis prevalence was 4.5%: The 95% confidence interval was 3.6% to 5.5%, with substantial variation across studies.
- Neuropsychiatric SLE carried a higher burden: Among patients already classified with neuropsychiatric SLE, psychosis prevalence was estimated at 20.5%.
- Immune activity mattered: Psychosis was linked with higher SLE disease activity, anti-ribosomal P antibodies, antiphospholipid antibodies, and complement consumption.
- A negative anti-ribosomal P result carried the clearest clue: The marker had high specificity and negative predictive value but low sensitivity.
Source: Parperis et al. Lupus. 2026.
Psychosis in lupus sits at an uncomfortable intersection. It can look psychiatric, but the biology may be autoimmune, vascular, medication-related, or some combination of those factors.
This review focused on that attribution problem. Researchers pooled evidence on adults with systemic lupus erythematosus, an autoimmune disease that can affect the nervous system, and asked how often psychosis appears and which clinical clues point toward lupus-related disease activity.
This review should not be read as saying that most psychosis is caused by lupus.
It says something narrower and clinically important: when a person already has SLE, new hallucinations, delusions, disorganized thinking, mania-like symptoms, or paranoia may need a medical and immune-disease workup, not only a psychiatric label.
Psychosis Was Uncommon in All SLE but Commoner in Neuropsychiatric SLE
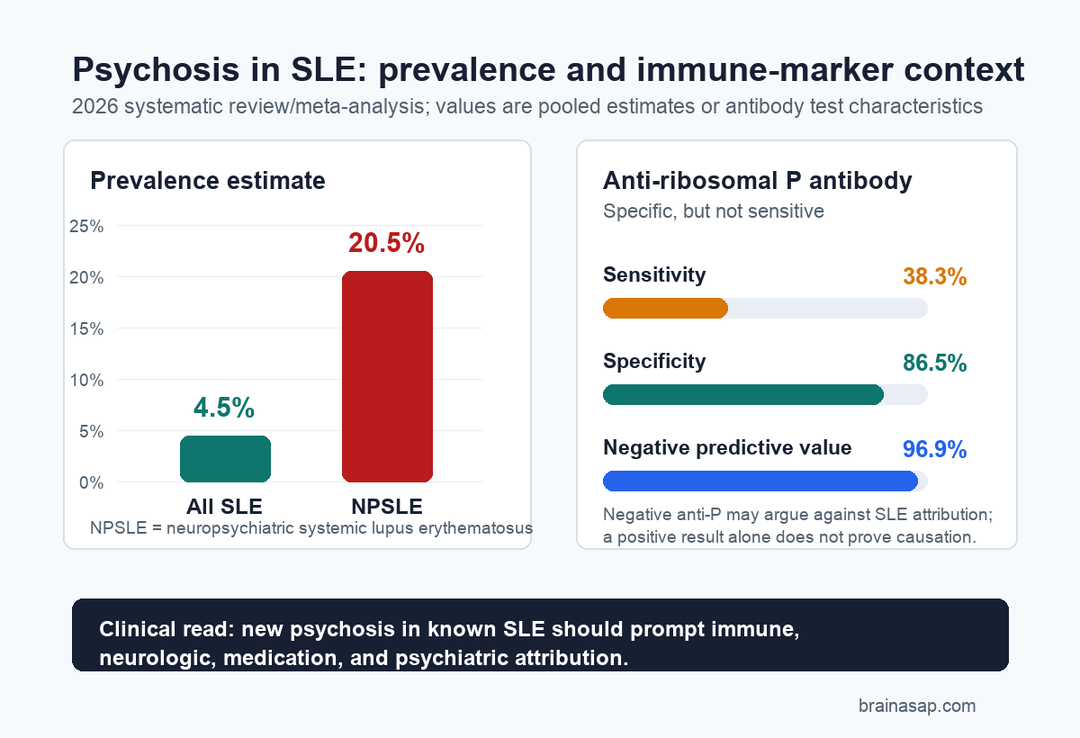
The meta-analysis included 65 studies and 31,495 SLE patients. Across the broader SLE population, the pooled prevalence of psychosis was 4.5%, with a 95% confidence interval from 3.6% to 5.5%.
That number is low enough that psychosis is not an expected feature of lupus for most patients. It is also high enough that clinicians cannot dismiss it as unrelated by default when it appears in someone with active or newly diagnosed SLE.
The rate changed sharply when the denominator was narrowed to neuropsychiatric SLE (NPSLE), the lupus subgroup with nervous-system or psychiatric involvement. In eight studies with 926 NPSLE patients, the pooled psychosis prevalence was 20.5%, although the confidence interval was wide at 10.0% to 37.6%.
- All SLE: Psychosis was estimated at 4.5% across the included adult SLE literature.
- NPSLE subgroup: Psychosis was estimated at 20.5% among patients already classified with neuropsychiatric lupus.
- Study variation: Heterogeneity was high, meaning definitions, populations, and attribution rules differed substantially.
The heterogeneity is a real limitation. The review pooled older and newer studies, multiple countries, and different diagnostic approaches.
The headline prevalence is informative, but it is not a single clean risk prediction for every clinic or patient.
Timing Pointed Toward Early Disease Vigilance
Several included studies reported that lupus-associated psychosis often appeared early in the disease course. Some patients had psychosis near SLE onset, and many episodes clustered within the first year or two after diagnosis.
That early timing fits the review’s larger interpretation. Psychosis seemed more likely when the immune disease was active, not simply when a person had a long-standing lupus history.
The symptoms themselves were not exotic. Studies that described presentation most often reported delusions and hallucinations, including paranoid delusions, auditory hallucinations, visual hallucinations, disorganized thinking, catatonia, and bizarre behavior in some reports.
New psychosis should not be used to self-diagnose lupus.
In someone with known SLE, though, it can be a red-flag presentation that belongs in the same conversation as inflammation, medications, seizures, vascular events, and other neurologic findings.
Immune Markers Were the Main Clinical Clue
The strongest pattern was immune activity. The review linked SLE psychosis with higher disease activity, anti-ribosomal P antibodies, antiphospholipid antibodies, and low complement markers such as C3, C4, or CH50 in some studies.
Anti-ribosomal P, often shortened to anti-P, received the most detailed discussion. Across studies that reported testing, anti-P antibodies were present in 38.3% of psychotic SLE patients tested, compared with 13.5% of non-psychotic SLE patients tested.
That difference supports a real association, but it does not make anti-P a simple diagnostic switch.
The review reported that anti-P had low sensitivity and low positive predictive value, meaning many lupus psychosis cases would not be captured by the marker and a positive result alone does not prove causation.
Its strength was the other direction. Anti-P showed 86.5% specificity and 96.9% negative predictive value in the summarized data, so a negative result may argue against psychosis being attributable to SLE in some clinical contexts.
- Anti-P antibodies: More common in SLE psychosis, but not sensitive enough to rule in the condition alone.
- Antiphospholipid antibodies: Linked in several studies, possibly through vascular or blood-brain-barrier mechanisms.
- Complement consumption: Low complement levels aligned with active immune-complex biology in some cohorts.
- Disease activity: Higher SLE activity repeatedly appeared as a risk marker.
This is why the review framed lupus psychosis as multifactorial. The same patient may need evaluation for autoimmune inflammation, vascular complications, corticosteroid exposure, seizures, infection, substance effects, primary psychiatric illness, and medication side effects.
Steroid Psychosis Remained a Separate Attribution Problem
Corticosteroids can also cause psychiatric symptoms, including psychosis. That creates a hard clinical problem because corticosteroids are also used to treat severe lupus activity.
The review noted that at least one study attempted to separate primary SLE psychosis from corticosteroid-induced psychosis. In that comparison, primary SLE psychosis was more associated with other central nervous system symptoms, while steroid-related episodes needed a different attribution frame.
The distinction has direct treatment implications.
If symptoms are driven by active neuropsychiatric lupus, clinicians may consider immunosuppression. If symptoms are driven by steroid exposure, increasing steroid intensity could worsen the problem.
The review did not solve that dilemma. It shows why careful attribution is necessary before treatment decisions are made.
The Evidence Is Useful but Not Uniform
The study’s main limitation is the uneven source literature. The included studies used different definitions for SLE psychosis, different neuropsychiatric lupus frameworks, different antibody panels, and different thresholds for attributing psychiatric symptoms to lupus rather than another cause.
The review also found high heterogeneity in several pooled estimates. That means the exact percentage should be treated as a map of the literature, not a universal bedside probability.
Still, the direction is coherent. Psychosis in SLE is uncommon overall, more prominent inside neuropsychiatric lupus, often appears early, and repeatedly tracks with immune dysregulation.
- Most SLE patients will not develop psychosis: The pooled all-SLE estimate was under 5%.
- New symptoms deserve medical context: Psychosis in known SLE can reflect active disease, vascular involvement, medication effects, or overlapping neurologic illness.
- Biomarkers are adjuncts: Anti-P, antiphospholipid antibodies, and complement levels can guide evaluation but do not replace clinical attribution.
The strongest takeaway is not that one blood test identifies lupus psychosis. It is that psychosis in SLE should be evaluated as a brain-and-immune event until the evidence points elsewhere.
Citation: DOI: 10.1177/09612033261432704. Study authors et al. Psychosis in patients with systematic lupus erythematosus: A systematic literature review and meta-analysis. Lupus. 2026.
Study Design: PRISMA-guided systematic review and random-effects meta-analysis of adult SLE studies that reported psychosis prevalence, features, or risk factors.
Sample Size: Sixty-five studies including 31,495 adults with systemic lupus erythematosus.
Key Statistic: Pooled psychosis prevalence was 4.5% in all SLE patients and 20.5% among neuropsychiatric SLE patients; anti-P antibodies showed 86.5% specificity and 96.9% negative predictive value.
Caveat: Study definitions and attribution rules varied widely, so the pooled estimates should not be treated as a single patient-level prediction.