TL;DR: A 2026 study in Drug and Alcohol Review found that laypeople reported more and better-developed cues for alcohol intoxication than cannabis intoxication, even though most coded cues for both substances were accurate.
Key Findings
- Intoxication-cue sample: The survey sample was 77.7% female, with an average age of 20.5 years, and came from undergraduate psychology students at the University of Sydney.
- 81.3% rated alcohol easy: Alcohol intoxication detection was rated somewhat easy by 52.0% and extremely easy by 29.3% of participants.
- Cannabis difficulty varied: Cannabis intoxication detection was most often rated somewhat difficult (33.2%), with 18.6% rating it extremely difficult and 18.6% somewhat easy.
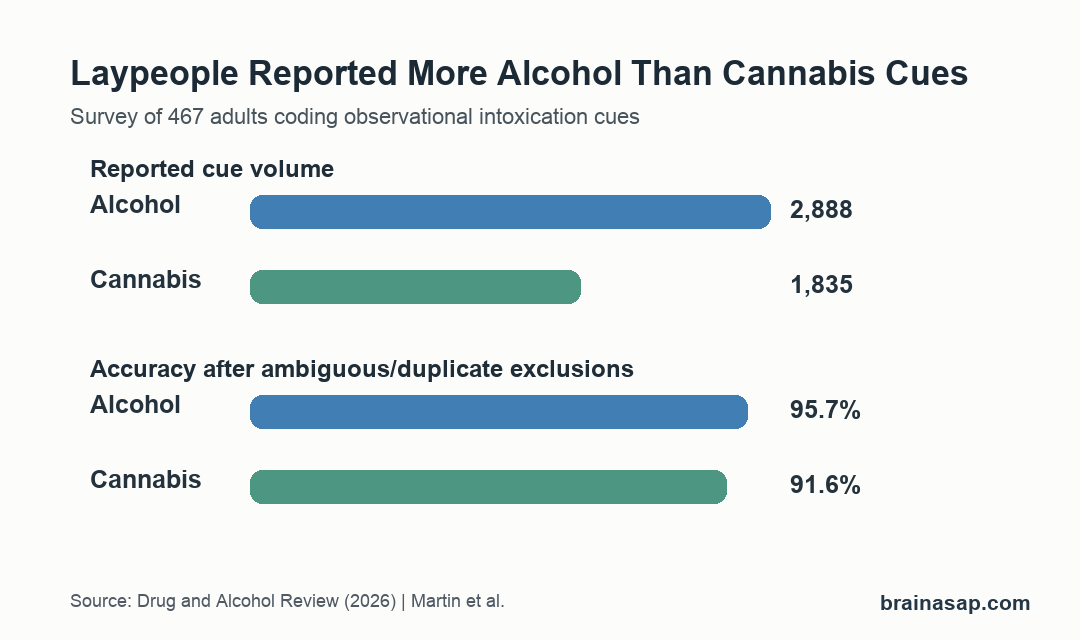
- 2,888 alcohol cues: Participants generated more reported cues for alcohol intoxication than cannabis intoxication, including more accurate cues.
- 91.6% cannabis-cue accuracy: After exclusions, 95.7% of alcohol cues and 91.6% of cannabis cues were coded as accurate, but non-responses showed knowledge gaps.
Source: Drug and Alcohol Review (2026) | Martin et al.
Intoxication detection often depends on visible behavior: speech, movement, eyes, alertness, mood, and smell. This study asked participants which observable cues they use to detect alcohol and cannabis intoxication, then coded those cues for accuracy.
Participants usually named accurate cues when they responded, but they had a thinner cue set for cannabis than for alcohol.
Survey Participants Listed Observable Intoxication Cues
The study used a survey of 467 participants from the University of Sydney. The sample was 77.7% female and had a mean age of 20.5 years, with an age range from 18 to 53.
Participants reported cues they would use to decide whether someone was intoxicated with alcohol or cannabis. They also rated how difficult that detection felt.
- Alcohol familiarity: The survey asked about alcohol use, alcohol-related work, and training related to serving or selling alcohol.
- Cannabis familiarity: Participants reported cannabis use and familiarity with cannabis effects.
- Cue coding: Responses were coded as accurate, partially accurate, inaccurate, ambiguous, subjective, or duplicate at the participant level.
- Predictor tests: The analysis examined whether personal characteristics predicted cue accuracy.
This was not a test of real-time detection from videos or live behavior. It measured what people say they look for when judging intoxication by observation.
Alcohol Intoxication Felt Easier to Identify
Most participants saw alcohol intoxication detection as straightforward. A combined 81.3% rated it either somewhat easy or extremely easy.
The common alcohol cue categories matched familiar signs: impaired speech, impaired motor control, other speech changes, and behavior. Examples included slurred speech, difficulty walking or standing, and smell of alcohol on breath.
- Somewhat easy: 52.0% selected this rating for alcohol intoxication detection.
- Extremely easy: 29.3% selected this rating.
- High cue volume: Participants generated 2,888 alcohol-cue responses before exclusions.
After ambiguous, subjective, or duplicate responses were removed, the remaining 2,557 alcohol cues were usually accurate. The accuracy-coded set was 95.7% accurate, 3.8% partially accurate, and 0.6% inaccurate.
Cannabis Intoxication Had More Knowledge Gaps
Cannabis intoxication detection did not have the same consensus. The most common rating was somewhat difficult at 33.2%, followed by neither easy nor difficult at 19.9%.
Participants generated 1,835 cannabis-cue responses, fewer than for alcohol. After exclusions, 1,627 responses remained for accuracy coding.
- Accurate cannabis cues: 91.6% were coded as accurate, including examples such as red eyes and slowed reactions.
- Partially accurate cues: 5.8% were partially accurate, including broad responses such as coordination or smell.
- Inaccurate cues: 2.6% were inaccurate, including examples such as looking emaciated or touching surfaces.
- Common categories: The most reported cannabis cue categories involved eyes, behavior, mood, and alertness.
Monthly or less-than-monthly cannabis consumption was associated with greater cannabis-cue accuracy compared with never using cannabis. Participants who rated cannabis detection as extremely difficult reported less accurate cannabis cues.
Non-Responses Changed the Meaning of High Accuracy
The headline accuracy percentages can sound reassuring, but the authors also examined non-responses. When non-responses were included to assess the breadth of knowledge, the proportion of accurate cues dropped substantially for both substances.
That distinction changes how the accuracy numbers should be read. A person may know a few correct cues but still miss many other signs in a high-risk setting, so the paper emphasized knowledge breadth as well as technical correctness.
- Healthcare settings: Staff may need to judge intoxication when symptoms, injury, or distress overlap with substance effects.
- Road and workplace safety: Observers may need to decide whether someone is safe to drive, operate equipment, or continue work.
- Criminal justice contexts: Witness credibility, consent, and behavior interpretation can depend on intoxication judgments.
The study suggests that education should include a broader range of observable cues, especially for cannabis. It should also avoid implying that one or two visible signs are enough for a reliable judgment.
The Study Measured Reported Knowledge, Not Real-Time Accuracy
The main limitation is that participants described cues in a survey. They did not watch intoxicated people, rate videos, or estimate intoxication dose.
That means accurate cue knowledge may not translate into accurate real-world detection. A person can name slurred speech or red eyes and still misread someone in a noisy bar, workplace, clinic, or roadside context.
- Sample limits: The sample was mostly young, female, and university based.
- Dose limits: The study did not test whether cues distinguish low, moderate, and severe intoxication.
- Substance specificity: Some cues can overlap with fatigue, illness, medication effects, or distress.
- Observation gap: Rote cue knowledge is not the same as detection skill under real conditions.
The direct interpretation is narrower: laypeople can name many correct cues, especially for alcohol, but cannabis cue knowledge is thinner and may need more targeted education in safety-critical settings.
Citation: DOI: 10.1111/dar.70156. Martin et al. What Cues Do Laypeople Use to Detect Alcohol and Cannabis Intoxication? Drug and Alcohol Review. 2026;45:e70156.
Study Design: Survey study of reported observational cues for alcohol and cannabis intoxication, with researcher-coded cue accuracy categories.
Sample Size: 467 participants, 77.7% female, from an undergraduate psychology sample in Australia.
Key Statistic: After exclusions, 95.7% of alcohol cues and 91.6% of cannabis cues were coded accurate, but participants generated more cues for alcohol than cannabis.
Caveat: The study measured reported cue knowledge, not real-time detection accuracy from observed intoxicated behavior.