TL;DR: A 2026 study in Interactive Journal of Medical Research used structured hospital records plus natural language processing of clinical notes to profile major depressive disorder in Belgium, finding that 46% of 1,147 adults met a real-world treatment-resistant depression definition.
Key Findings
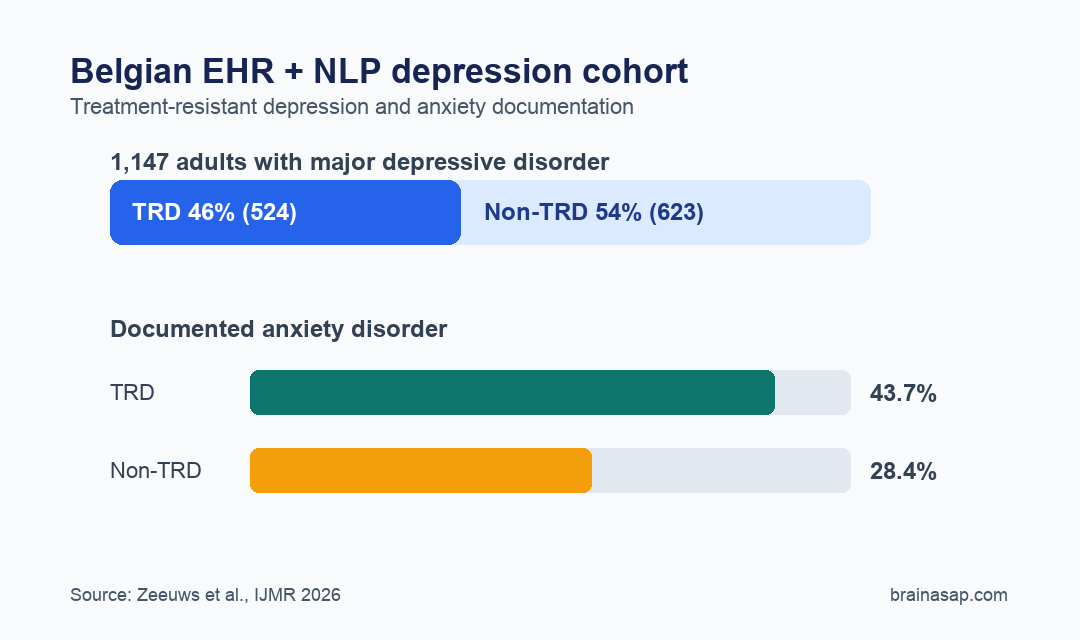
- Belgian EHR cohort: The retrospective study drew from 1,147 adults with major depressive disorder at 2 Belgian hospitals between September 2021 and June 2023.
- 46% met TRD criteria: Treatment-resistant depression was identified in 524 of 1,147 patients, mostly through medication sequencing rather than explicit TRD labels in notes.
- 43.7% anxiety in TRD: Anxiety disorder was recorded in 229 of 524 TRD patients versus 177 of 623 non-TRD patients, or 28.4%.
- 14.8% severe MDD recorded: Severe major depressive disorder was documented in 170 of 1,147 patients, but standardized severity scales were rarely captured.
- 56,396 records processed: The natural language processing workflow converted free-text clinical documentation into standardized concepts for real-world psychiatric analysis.
Source: Interactive Journal of Medical Research (2026) | Zeeuws et al.
Major depressive disorder (MDD) is easy to name in a diagnosis code and hard to characterize from routine records. Severity, relapse, partial response, suicidal thoughts, medication reasons, and functional context often live in clinician notes rather than structured fields.
This study tested a practical psychiatric data problem: whether natural language processing (NLP), a method for extracting structured meaning from free text, can make real-world depression records more useful without asking clinicians to rebuild their workflow.
Belgian EHR Data Identified 524 Treatment-Resistant Depression Cases
Researchers analyzed electronic health records from University Hospital Brussels and Psychiatric Center Ariadne. The study included adults with MDD documented by diagnostic codes or NLP-detected note mentions, while bipolar depression was excluded.
Treatment-resistant depression (TRD) was defined operationally as initiation of a third distinct antidepressant, supplemented by explicit TRD mentions in unstructured notes. That definition favors sensitive real-world identification, but it cannot always separate nonresponse from intolerance or other reasons for medication changes.
- MDD cohort: 1,147 adults with major depressive disorder.
- TRD subgroup: 524 patients, or 46% of the MDD cohort.
- Non-TRD subgroup: 623 patients, or 54% of the cohort.
- Explicit TRD notes: Only 8 TRD patients had a direct TRD mention; most were identified by antidepressant sequencing.
The high TRD proportion fits a hospital-based depression population better than a general community sample. The cohort was drawn from specialized care settings where more complex and persistent cases are expected.
Anxiety and Dementia Were More Common in the TRD Subgroup
The patient profile showed why TRD is more than a medication-count label. Psychiatric comorbidities were heavier in the TRD group, especially anxiety disorder.
Anxiety disorder appeared in 43.7% of TRD patients compared with 28.4% of non-TRD patients. Personality disorder was also higher in TRD, at 12.2% versus 7.1%.
- Dementia: 42 of 524 TRD patients, or 8.0%, versus 32 of 623 non-TRD patients, or 5.1%.
- Central nervous system diseases: 477 of 1,147 patients overall, or 41.6%.
- Heart diseases: 349 of 1,147 patients overall, or 30.4%.
- Suicidal history: 334 of 1,147 patients overall, or 29.1%.
Obesity moved in the other direction: 11.2% in non-TRD versus 8.8% in TRD. The descriptive design supports cautious comparison rather than a protective interpretation.
NLP Filled Some Gaps That Diagnosis Codes Missed
The paper’s main contribution is methodological. Researchers combined structured fields, such as diagnoses, medications, and hospitalizations, with unstructured text from clinician notes, pathology reports, and other documentation.
The NLP pipeline split documents into sentences and words, identified clinical entities, linked them to standardized medical concepts, and classified context such as negation, uncertainty, family history, and timing.
That context handling is crucial in psychiatry because a phrase such as “no suicidal ideation” should not become a false positive suicidal-ideation record.
- Entity recognition: The system identified clinical terms such as remission, relapse, symptoms, diagnoses, and medications.
- Attribute handling: It separated affirmed findings from negated, historical, hypothetical, or family-context mentions.
- Concept mapping: Extracted terms were normalized to standard vocabularies used in the Observational Medical Outcomes Partnership common data model.
Medication context shows the problem clearly. Trazodone and benzodiazepines can appear in psychiatric records for sleep, anxiety, or other purposes.
Structured medication data alone may not show the intended clinical use, while note context can.
Depression Severity Documentation Was Still Too Sparse
The same system also exposed an important weakness in psychiatric records: standardized severity measurement was uncommon. Severe MDD was documented in 170 of 1,147 patients, or 14.8%, while the remaining records often lacked enough standardized scale detail for severity grading.
The authors note that severity scales such as the Montgomery-Asberg Depression Rating Scale (MADRS) and Clinical Global Impressions-Severity (CGI-S) were rarely recorded. When scales are absent, an NLP system can extract descriptors, but it should not invent severity scores.
- Clinical documentation gap: Severity was often captured in narrative terms rather than standardized scales.
- TRD definition gap: Medication sequencing cannot always identify whether a drug change reflected nonresponse, adverse effects, or patient preference.
- Generalizability gap: The data came from 2 Belgian hospitals, so broader networks are needed before assuming the same profile elsewhere.
For research, this is a concrete warning. Artificial intelligence can organize messy records, but it cannot fully repair missing clinical measurement.
Real-World Psychiatry Needs Cleaner Inputs, Not Just Smarter Models
The study supports a practical middle ground for AI in mental-health research. NLP can reduce manual chart-review burden and recover clinically specific details from text, but its value depends on what clinicians document.
The highest-yield improvement may be small: recording standardized severity scores and treatment-change reasons more consistently. That would make future TRD analyses more clinically meaningful than medication sequencing alone.
For patients with MDD and TRD, the paper is an evidence-infrastructure study rather than a treatment test. It builds the record system for later treatment-pattern and outcome studies, including esketamine analyses planned within the broader MOOD project.
The immediate lesson is operational: real-world evidence in psychiatry will work best when structured data, clinician notes, standardized scales, and patient-reported outcomes are treated as complementary sources instead of substitutes for one another.
Citation: DOI: 10.2196/86448. Zeeuws et al. Real-World Clinical Characterization of Major Depressive Disorder and Treatment-Resistant Depression Using Natural Language Processing: Multicenter Observational Study From the MOOD Project. Interactive Journal of Medical Research. 2026;15:e86448.
Study Design: Retrospective multicenter observational EHR study using structured data plus NLP of free-text records.
Sample Size: 1,147 adults with MDD from 2 Belgian hospitals; 524 met the study’s TRD definition.
Key Statistic: TRD accounted for 46% of the MDD cohort, and anxiety disorder was documented in 43.7% of TRD patients versus 28.4% of non-TRD patients.
Caveat: TRD was mostly inferred from antidepressant sequencing, and standardized depression severity scores were rarely recorded.