TL;DR: A 2026 nationwide claims study in Integrative Medicine Research found that Korean traditional medicine care without recorded acupuncture claims had the lowest modeled costs and the highest 3-year QALYs among four menopausal-disorder treatment strategies, while acupuncture and integrative-care groups appeared to include sicker, higher-utilization patients.
Key Findings
- 32,941 women: The retrospective cohort used Korean National Health Insurance claims from 2015 to 2023 for women with menopausal disorders.
- Four care strategies: Researchers compared traditional Korean medicine (TKM) without acupuncture claims, TKM with acupuncture, TKM plus Western medicine, and TKM plus Western medicine with acupuncture.
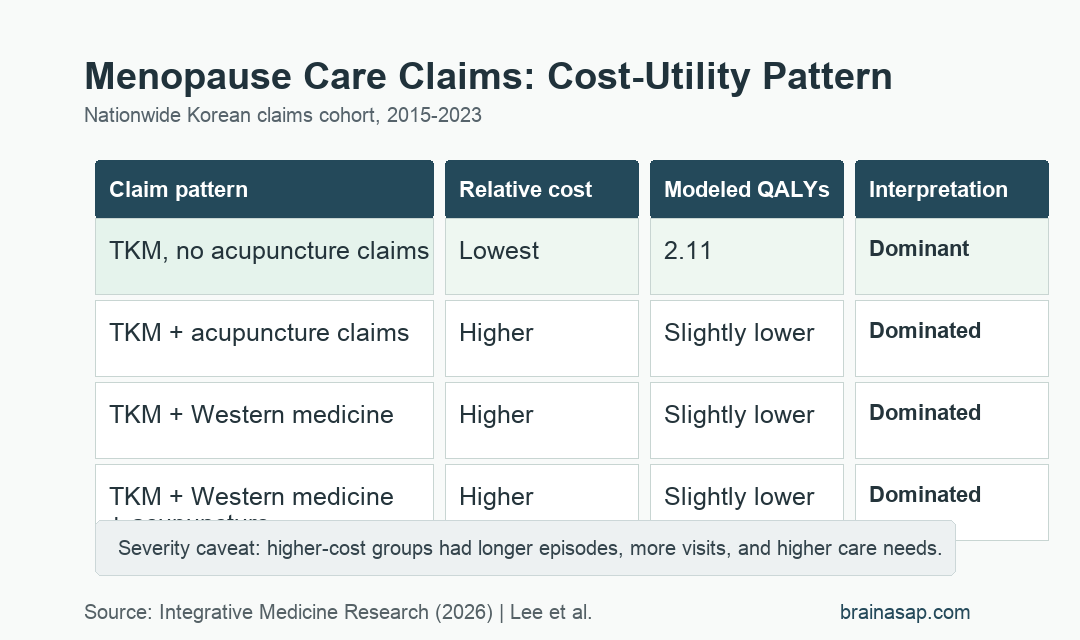
- 2.11 QALYs: The TKM-without-acupuncture-claims group had the highest modeled 3-year quality-adjusted life years and the lowest cost profile.
- Dominated alternatives: All three acupuncture or Western-medicine integration strategies were classified as dominated because they had higher costs and slightly lower QALYs.
- Severity caveat: Acupuncture users had longer treatment episodes, more visits, and higher comorbidity burden, so the results should not be read as proof that acupuncture itself performed worse.
Source: Integrative Medicine Research (2026) | Lee et al.
Menopausal disorders often combine physical symptoms with mood and sleep problems, including depression symptoms that can lower quality of life. This study asked a narrower health-economics question: among women already using Korean insurance-covered care, which treatment-claim pattern looked most cost-effective over 3 years?
The comparison was not a simple treatment ranking. The lower-cost group was also the group with shorter episodes and fewer recorded visits, so patient severity remains central to the interpretation.
Korean Claims Data Compared Four Menopause Treatment Patterns
The analysis used nationwide Korean National Health Insurance data from 2015 to 2023. Researchers identified women with menopausal-disorder diagnoses and followed depression incidence and modeled quality-adjusted life years (QALYs), a measure that combines survival time and health-related quality of life.
The four groups were defined by recorded claims rather than randomized assignment. A claim pattern can reflect the kind of care a patient needed, the severity of symptoms, and the clinician or patient preference behind treatment selection.
- TKM without acupuncture claims: This was the reference group and included traditional Korean medicine care without recorded acupuncture claims.
- TKM plus acupuncture claims: This group added acupuncture claims to the traditional Korean medicine record.
- TKM plus Western medicine: This group had both traditional Korean medicine and Western medicine claims but no acupuncture claims.
- TKM plus Western medicine plus acupuncture: This was the most integrated pattern, combining all three claim categories.
Because the study was observational, researchers used inverse probability of treatment weighting to balance measured baseline differences. After weighting, most covariates reached the usual balance target of standardized mean difference below 0.1, although hormone therapy use remained less balanced.
TKM Without Acupuncture Claims Had the Best Modeled Cost-Utility Result
The main result favored the simplest claim pattern. The group receiving TKM without acupuncture claims had the lowest costs and the highest modeled QALYs, reported as 2.11 QALYs over the 3-year horizon.
In health-economics terms, the other three strategies were described as dominated. A dominated strategy costs more and produces less health benefit than the comparator, so it is not considered economically attractive in that model.
- Acupuncture-claim group: TKM plus acupuncture had higher costs and slightly lower QALYs than the reference group.
- Western-medicine group: TKM plus Western medicine without acupuncture also had higher modeled costs and lower QALYs.
- Fully integrated group: TKM plus Western medicine plus acupuncture had the highest-intensity claim pattern and was also dominated in the base-case model.
- Sensitivity checks: The reference group remained dominant when the researchers varied utility values by 20% and tested discount rates of 0%, 3%, and 7.5%.
The probabilistic analysis supported the same conclusion. Across willingness-to-pay thresholds up to KRW 30 million per QALY, the TKM-without-acupuncture-claims group had the highest probability of being cost-effective.
Acupuncture Groups Looked Sicker and Used More Care
The strongest caution is built into the baseline table. Acupuncture users were not simply interchangeable with non-users.
The fully integrated TKM plus Western medicine plus acupuncture group had the longest menopausal-disorder episode duration and the most visits.
Before weighting, the reference group had a mean episode duration of 17.39 days, while the fully integrated group averaged 966.38 days. Visit counts also differed sharply, from 1.47 visits in the reference group to 19.49 visits in the fully integrated group.
- Care intensity: More visits may signal more persistent vasomotor, sleep, pain, or mood symptoms.
- Comorbidity burden: Musculoskeletal symptoms were common overall and especially frequent in higher-utilization groups.
- Hormone therapy imbalance: Hormone replacement therapy claims were far more common in Western-medicine groups, which complicates direct interpretation.
The claims model favored TKM without acupuncture claims economically, but it did not prove that acupuncture caused lower QALYs or higher costs.
Depression Was Modeled Through Claims, Not Symptom Interviews
Depression was defined by ICD-10 diagnosis codes for depressive episodes or recurrent depressive disorder during follow-up. The outcome works for large insurance-data analysis, but it differs from repeated symptom-scale measurement.
The study estimated QALYs because direct quality-of-life questionnaires such as EQ-5D were not available in the claims database. Utility values therefore came from published estimates rather than from each woman in the cohort.
- Depression outcome: Incident depression was based on recorded F32 or F33 diagnosis codes.
- Health utility: QALYs were modeled from external utility values and event timing.
- Economic horizon: Costs and effects were modeled over 3 years, discounted at 4.5% in the base case.
- Unmeasured symptoms: Hot flashes, insomnia severity, patient preference, and treatment response could not be fully captured from claims.
Menopause-related depression symptoms are clinically personal. Claims can show utilization and coded outcomes at scale.
They cannot fully show whether one woman slept better, felt less anxious, or chose acupuncture because earlier care had failed.
Claims-Based Menopause Care Results Need Prospective Follow-Up
In this dataset, the lowest-intensity TKM claim pattern was the most economically favorable. More complex integrative care was associated with higher costs and slightly lower modeled QALYs.
For clinicians and patients, the finding should function as a triage and research prompt rather than a care directive.
Women with more severe symptoms may naturally move into more intensive treatment patterns, and those patients may need different support than women with shorter, less complex episodes.
A prospective study could measure menopausal symptoms, sleep, depression scales, treatment preference, and adverse effects directly. That would help separate treatment effect from the severity patterns that claims data can only partly adjust.
Citation: DOI: 10.1016/j.imr.2026.101315. Lee et al. Cost-utility analysis of traditional Korean medicine without acupuncture claims versus integrative care for menopausal disorders: A nationwide retrospective cohort study. Integrative Medicine Research. 2026;15:101315.
Study Design: Nationwide retrospective claims-based cost-utility analysis using Korean National Health Insurance data.
Sample Size: 32,941 women with menopausal-disorder claims from 2015 to 2023.
Key Statistic: TKM without acupuncture claims had the lowest costs and highest modeled QALYs, reported as 2.11 over 3 years; the other three strategies were dominated.
Caveat: The study was observational, and higher-cost integrative-care groups appeared to include patients with longer episodes and greater care needs.