TL;DR: A 2026 randomized trial in Nature and Science of Sleep found that Sancai acupoint acupuncture reduced primary-insomnia severity more than sham acupuncture, with parallel improvements in sleep testing and peripheral 5-HT and BDNF biomarkers.
Key Findings
- 76-person insomnia trial: Researchers randomized 38 patients to real Sancai acupuncture and 38 to sham acupuncture.
- 20 treatment sessions: Real acupuncture was delivered over 8 weeks, three times weekly during weeks 1-4 and twice weekly during weeks 5-8.
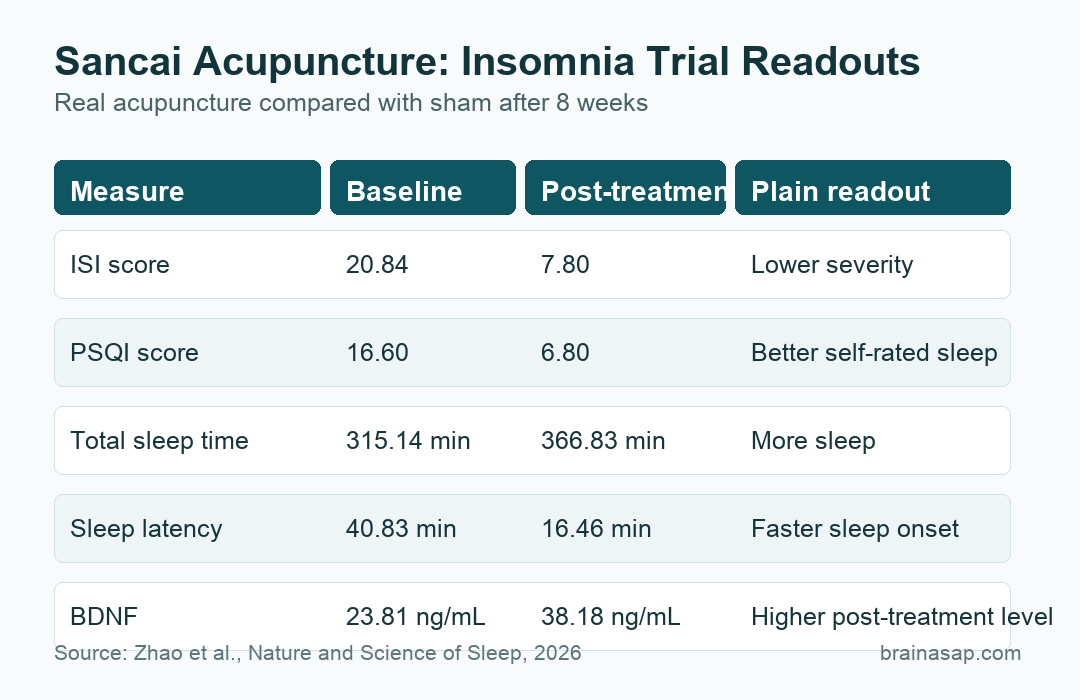
- Insomnia severity fell: Real-acupuncture Insomnia Severity Index scores dropped from 20.84 to 7.80 after treatment, compared with 21.58 to 16.45 in the sham group.
- Sleep testing improved: After treatment, real acupuncture showed longer total sleep time, higher sleep efficiency, shorter sleep latency, lower wake after sleep onset, and more N3 slow-wave sleep.
- Biomarkers increased: Serum 5-HT reached 101.91 ng/mL and BDNF reached 38.18 ng/mL after real acupuncture, both higher than sham values.
Source: Nature and Science of Sleep (2026) | Zhao et al.
Sancai acupoint acupuncture was tested as a structured treatment for primary insomnia, meaning persistent insomnia not explained by another primary sleep disorder. The useful part of this trial is that it did not rely only on questionnaires.
Researchers also used polysomnography (PSG), an overnight sleep test, and measured peripheral 5-hydroxytryptamine (5-HT) and brain-derived neurotrophic factor (BDNF). That gives the paper subjective, objective, and biomarker readouts, although the biomarker results remain exploratory.
Sancai Acupuncture Used Head, Chest, Back, and Foot Points
The trial enrolled adults ages 18-65 with primary insomnia at Yueyang Hospital of Integrated Traditional Chinese and Western Medicine in Shanghai. Participants were randomized to real acupuncture or sham acupuncture and followed through 12 weeks after treatment.
The Sancai protocol came from a traditional “heaven, human, earth” framework, but the clinical comparison was ordinary: real needling versus non-penetrating sham needling at the same acupoint locations.
- Heaven domain: Baihui (GV20) and Shenting (GV24) on the head.
- Human domain: Xinshu (BL15) and Danzhong (CV17) on the back/chest region.
- Earth domain: Taibai (SP3) and Taichong (LR3) on the feet.
- Schedule: Each session retained needles for 30 minutes, with 20 sessions across 8 weeks.
Participants, outcome assessors, PSG scorers, laboratory personnel, and the data analyst were blinded to allocation. Acupuncturists could not be blinded because they delivered the intervention.
Insomnia Severity Index Scores Dropped Below the Clinical Range
The primary outcome was the Insomnia Severity Index (ISI), where higher scores indicate worse insomnia and scores above 14 indicate clinically significant insomnia. At baseline, the real-acupuncture group averaged 20.84 and the sham group averaged 21.58.
After treatment, the real-acupuncture group averaged 7.80, while the sham group averaged 16.45. The between-group difference was significant at post-treatment, with a standardized mean difference of 2.130.
- Primary time point: The week-8 ISI comparison was the only confirmatory efficacy test in the paper.
- Clinical scale shift: The real-acupuncture mean moved from clinically significant insomnia to below the subthreshold range.
- Durability: ISI remained lower than sham at 1, 4, and 12 weeks after treatment.
That does not make acupuncture a replacement for cognitive behavioral therapy for insomnia (CBT-I), a first-line behavioral treatment. It does show a large short-term and follow-up symptom separation against a sham procedure in this setting.
PSQI and Polysomnography Pointed in the Same Direction
The Pittsburgh Sleep Quality Index (PSQI), a self-report sleep-quality scale, also improved. Real-acupuncture scores fell from 16.60 at baseline to 6.80 after treatment, while sham scores changed from 15.70 to 15.09.
Objective PSG results supported the same broad direction. After treatment, total sleep time was 366.83 minutes in the real-acupuncture group versus 287.97 minutes in the sham group.
- Sleep efficiency: Real acupuncture reached 76.75% after treatment, compared with 68.29% for sham.
- Sleep latency: Time to fall asleep was 16.46 minutes after real acupuncture, compared with 47.97 minutes after sham.
- Wake after sleep onset: Real acupuncture averaged 96.69 minutes, compared with 157.39 minutes after sham.
- Slow-wave sleep: N3 sleep reached 29.61% after real acupuncture, compared with 24.54% after sham.
REM latency did not separate between groups, and not every sleep-stage measure changed. The strongest objective signal was the combination of more total sleep, shorter latency, less wake time after sleep onset, and higher N3 sleep.
Anxiety Scores Lasted Longer Than Depression Scores
The trial also measured self-rated anxiety and depression. Anxiety scores showed a clearer follow-up separation than depression scores, which matters because insomnia often travels with emotional hyperarousal.
Self-Rating Anxiety Scale scores averaged 40.66 at 12-week follow-up in the real-acupuncture group versus 45.18 in sham. The 12-week between-group difference was significant, and the sensitivity analysis before imputation gave the same P value.
- Anxiety: Real acupuncture separated from sham at week 4 and week 12.
- Depression: Self-Rating Depression Scale scores separated at week 4 but not at week 12.
- Missing follow-up data: 2 real-acupuncture and 3 sham participants were lost at 12 weeks, and the trial used last-observation-carried-forward imputation.
The emotional-symptom results should be read as secondary. They moved in the same direction as the insomnia result, but they do not prove that the acupuncture protocol is a standalone anxiety or depression treatment.
5-HT and BDNF Increased After Real Acupuncture
Blood biomarkers were comparable at baseline. After treatment, serum 5-HT, a serotonin-related molecule involved in sleep-wake regulation, averaged 101.91 ng/mL after real acupuncture and 87.07 ng/mL after sham.
Serum BDNF, a neurotrophic factor involved in neural plasticity and mood regulation, averaged 38.18 ng/mL after real acupuncture and 24.78 ng/mL after sham. Both between-group biomarker comparisons were significant.
- Specificity caution: 5-HT also increased in the sham group, so not every biomarker change was acupuncture-specific.
- BDNF contrast: BDNF increased in the real-acupuncture group but not in the sham group.
- Mechanism boundary: Peripheral blood markers do not prove what happened inside the brain.
The biomarker data are useful because they give the trial a biological readout beyond symptom scales. They are not enough to identify the central nervous system pathway responsible for the sleep changes.
Mild Bruising Was the Main Safety Event
The safety profile was straightforward. 9 participants had skin bruising, all in the real-acupuncture group. The bruises were mild, required no medical intervention, and resolved within 2 weeks.
No bleeding, infection, dizziness, needle allergy, syncope, or serious adverse event was reported during treatment or follow-up. Blinding also looked acceptable: Bang’s index was 0.143 for real acupuncture and -0.077 for sham.
The main limitations are the single-center setting, modest sample size, incomplete 12-week follow-up data, and the impossibility of blinding acupuncturists. The biomarker findings also need larger trials that connect peripheral changes with brain activity or sleep-network measures.
Citation: DOI: 10.2147/NSS.S590127. Zhao et al. Acupuncture with the Sancai Acupoint Matching Method for Primary Insomnia: A Randomized Controlled Trial. Nature and Science of Sleep. 2026;18:590127.
Study Design: Single-center randomized, sham-controlled clinical trial with blinded participants, outcome assessors, PSG scorers, laboratory personnel, and data analyst.
Sample Size: 76 adults with primary insomnia, randomized 1:1 to real Sancai acupuncture or sham acupuncture.
Key Statistic: ISI scores fell from 20.84 to 7.80 after real acupuncture, compared with 21.58 to 16.45 after sham acupuncture.
Caveat: The trial was modest and single-center, and peripheral 5-HT/BDNF changes do not prove the central brain mechanism.