TL;DR: A 2026 ADNI analysis posted to medRxiv found that brain-derived plasma pTau217 better predicted near-term amyloid positron emission tomography (PET) positivity than total plasma pTau217 in cognitively unimpaired amyloid-negative participants.
Key Findings
- 1,427 ADNI participants: Plasma NULISAseq biomarkers were measured across the broader Alzheimer’s Disease Neuroimaging Initiative sample.
- 529 cognitively unimpaired: The main prognostic comparison focused on participants without cognitive impairment at baseline.
- 175 amyloid-negative: Amyloid PET progression was tested in cognitively unimpaired participants who were amyloid-negative at baseline.
- 0.82 vs 0.69 AUC: Brain-derived pTau217 outperformed total pTau217 for predicting amyloid PET positivity at 2.5 years.
- Similar clinical prediction: Brain-derived and total pTau217 performed more similarly for predicting progression to mild cognitive impairment or dementia.
Source: medRxiv (2026) | Gonzalez et al.
Phosphorylated tau 217, often shortened as pTau217, is one of the strongest blood biomarker families in Alzheimer disease research. The newer comparison is whether a brain-derived version, BD-pTau217, adds prognostic information beyond total plasma pTau217.
This ADNI analysis separated biological progression from clinical progression. Amyloid PET positivity is a brain-imaging marker of amyloid plaque burden, while mild cognitive impairment and dementia are clinical outcomes that can take longer to emerge.
Brain-Derived pTau217 Targeted Alzheimer Biology More Directly
Total plasma pTau217 can reflect Alzheimer-related tau biology, but blood measurements may include peripheral contributions. Brain-derived pTau217 aims to focus the assay on tau released from the central nervous system.
The study used NULISAseq plasma biomarkers in 1,427 ADNI participants. The main prognostic comparison centered on 529 cognitively unimpaired people, including a subset who were amyloid-negative at baseline and had longitudinal PET imaging.
- Biomarker comparison: Brain-derived pTau217 was compared directly with total plasma pTau217.
- Biological endpoint: Amyloid PET conversion measured movement from amyloid-negative to amyloid-positive status.
- Clinical endpoint: Progression to mild cognitive impairment or dementia tested whether the biomarker predicted symptoms.
- Risk-stratification use: The intended application is prevention-trial enrichment, not stand-alone diagnosis.
The design fits an early Alzheimer disease aim. In prevention studies, researchers need to identify cognitively unimpaired people who are biologically more likely to show amyloid progression during the study window.
Centiloid thresholds supplied the amyloid PET framework. The primary analysis used progression to PET positivity at the CL >= 24.1 threshold, a way of standardizing amyloid imaging burden across scans and tracers.
That endpoint is narrower than Alzheimer diagnosis. It asks whether a person crosses an imaging threshold, not whether daily memory, language, or function changes during the same period.
BD-pTau217 Predicted Amyloid PET Positivity Better Than Total pTau217
Among baseline amyloid-negative cognitively unimpaired participants, BD-pTau217 performed better for near-term amyloid PET progression. At 2.5 years, the time-dependent AUC was 0.82 for BD-pTau217 versus 0.69 for total pTau217.
At 4 years, BD-pTau217 still led, with AUC 0.77 versus 0.64 for total pTau217. Hazard ratios also favored the brain-derived marker, including HR 10.54 at 2.5 years and HR 7.03 at 4 years.
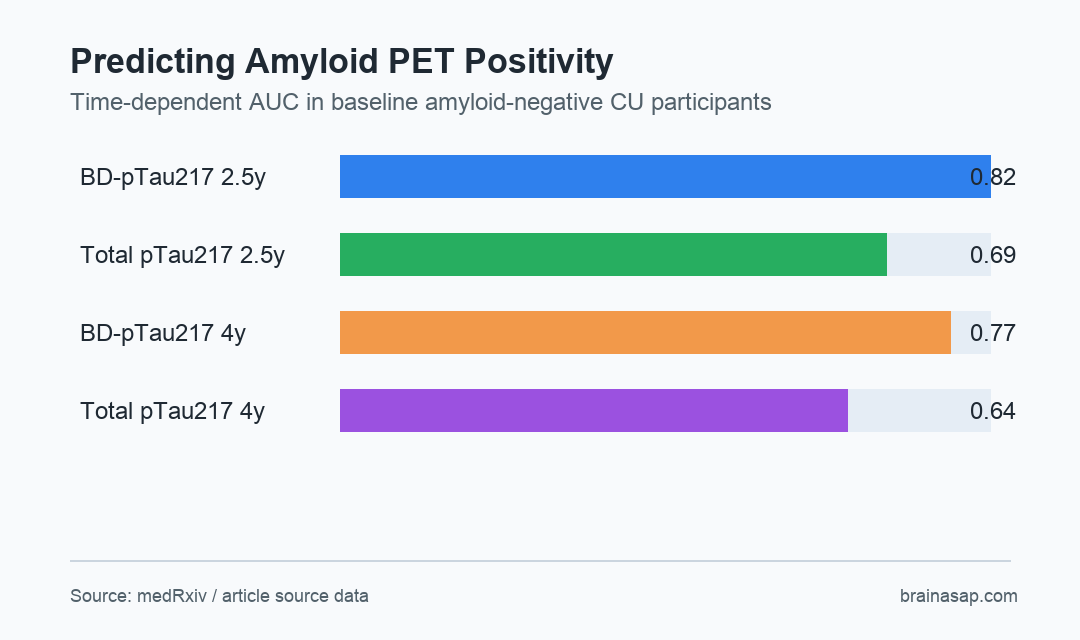
- 2.5-year prediction: BD-pTau217 reached AUC 0.82 versus 0.69 for total pTau217.
- 4-year prediction: BD-pTau217 reached AUC 0.77 versus 0.64 for total pTau217.
- Hazard ratios: BD-pTau217 showed strong associations with amyloid PET progression at both time windows.
These estimates support a specific use case: identifying who is likely to cross an amyloid PET threshold soon. That is different from telling an individual patient whether or when cognitive symptoms will develop.
The hazard ratios were large, and the subgroup was small enough to require replication. The amyloid-negative PET-progression analysis used 175 participants.
Clinical Progression Prediction Was Less Clearly Improved
The same advantage did not carry over as clearly to clinical progression. BD-pTau217 and total pTau217 performed more similarly for predicting progression from cognitively unimpaired status to mild cognitive impairment or dementia.
That difference fits Alzheimer biology. Amyloid PET positivity can change before overt clinical impairment.
Clinical progression depends on many additional factors, including tau spread, neurodegeneration, vascular disease, resilience, age, education, and follow-up duration.
- Better-supported endpoint: Near-term amyloid PET conversion.
- Less distinct endpoint: Clinical progression to mild cognitive impairment or dementia.
- Trial implication: BD-pTau217 may help enrich prevention studies for participants likely to show amyloid progression.
- Clinical caution: A biomarker that predicts PET conversion is not automatically a symptom forecast.
The analysis therefore supports a role for BD-pTau217 in biological risk stratification. It does not make total pTau217 obsolete, and it does not turn a blood test into a complete Alzheimer prognosis.
That distinction is especially important for prevention trials. A biomarker can be valuable for choosing trial participants even when it is not sufficient for counseling one person about future dementia.
The source therefore supports trial-enrichment use more strongly than routine clinical prognosis. That narrower role still helps researchers test prevention therapies before symptoms appear in trials.
Diverse Cohorts and Clinical-Grade Assays Remain Necessary
ADNI is a deeply characterized research cohort, which is a strength for biomarker studies. It is also not the same as a broad primary-care population, memory-clinic population, or globally diverse screening sample.
Assay platform also matters. A promising research biomarker must show stable performance across laboratories, pre-analytic handling conditions, clinical-grade platforms, racial and ethnic groups, comorbidities, and medication profiles.
For now, the claim is specific: brain-derived plasma pTau217 better predicted amyloid PET positivity in a cognitively unimpaired ADNI subgroup. The next test is whether that advantage holds in larger and more diverse prevention-trial screening pipelines.
Citation: DOI: 10.64898/2026.06.26.26356597. Gonzalez et al. Prognostic value of plasma brain-derived pTau. medRxiv. 2026.
Study Design: ADNI plasma biomarker prognostic analysis using Cox models and time-dependent AUC.
Sample Size: 1,427 ADNI participants overall, including 529 cognitively unimpaired participants and 175 baseline amyloid-negative participants for PET progression analysis.
Key Statistic: BD-pTau217 predicted amyloid PET positivity at 2.5 years with AUC 0.82 versus 0.69 for total pTau217.
Caveat: The biomarker advantage was clearer for amyloid PET progression than for clinical progression to mild cognitive impairment or dementia.