TL;DR: A 2026 human study in Biological Psychiatry: Global Open Science found that low-intensity focused ultrasound aimed at salience-network hubs improved early skin-conductance habituation to repeated startle sounds, while eye-blink and EEG habituation did not change.
Key Findings
- Forty healthy adults completed a crossover experiment: Participants attended separate low-intensity focused ultrasound (LIFU) sessions targeting the right anterior insula, right anterior midcingulate cortex, and sham stimulation.
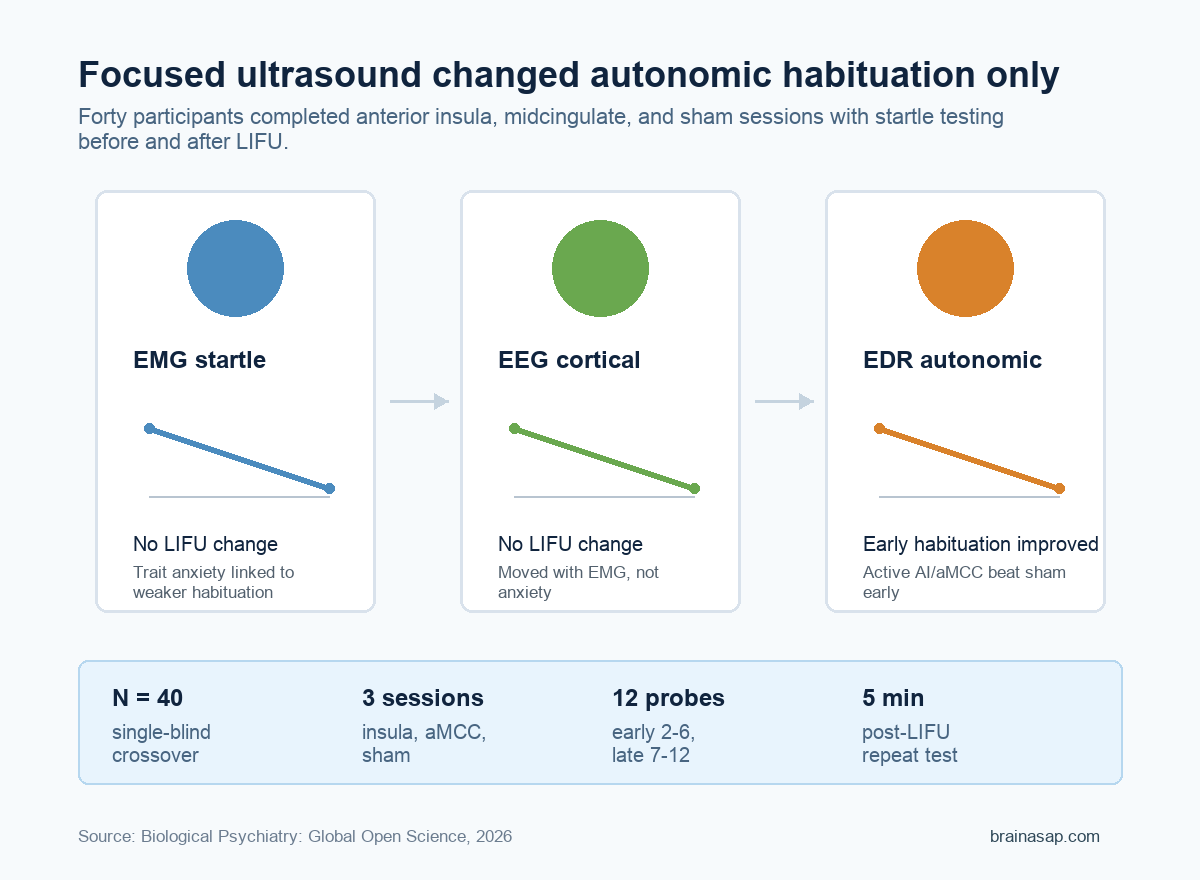
- The startle test used three body-brain readouts: Researchers measured eye-blink muscle activity with electromyography (EMG), cortical response with electroencephalography (EEG), and autonomic arousal with electrodermal response (EDR), a skin-conductance measure.
- Trait anxiety tracked weaker eye-blink habituation: Higher State-Trait Anxiety Inventory-Trait scores were associated with less reduction in EMG startle responses across early and late repeated sounds.
- Focused ultrasound selectively changed autonomic habituation: Active stimulation of the anterior insula or anterior midcingulate cortex enhanced early EDR habituation relative to sham, but did not significantly alter EMG or EEG habituation slopes.
- Body and brain signals split into different channels: EMG and EEG habituation moved together, while EDR habituation varied more independently, suggesting salience-network ultrasound affected autonomic adaptation rather than the whole startle system.
Repeated sounds normally become less biologically important after the body learns they are harmless. This study asked whether anxiety-relevant differences in that adaptation can be measured across muscle, brain, and skin-conductance signals, then briefly nudged with targeted ultrasound.
The result was specific rather than sweeping. Low-intensity focused ultrasound did not make every startle measure settle faster. It mainly shifted the autonomic channel, the skin-conductance response that reflects sympathetic arousal.
Forty Adults Completed Three Focused Ultrasound Sessions
The study used a single-blind, sham-controlled crossover design. Each participant completed three formal sessions on separate days: one targeting the right anterior insula, one targeting the right anterior midcingulate cortex, and one sham condition.
Those regions were chosen because they sit inside the salience and central-autonomic networks. The anterior insula helps integrate bodily readouts with uncertainty and subjective feeling states.
The anterior midcingulate cortex is tied to action selection, motivation, and context-dependent autonomic control.
During each session, researchers recorded responses to 12 acoustic startle probes. The same startle sequence was run before stimulation and again about 5 minutes after 40 seconds of LIFU.
- EMG: Eye-blink muscle activity captured the somatic startle reflex.
- EEG: Scalp electrical activity captured cortical response to the repeated sounds.
- EDR: Skin conductance captured sympathetic autonomic arousal.
Researchers analyzed habituation slopes separately for early trials 2-6 and late trials 7-12. A more negative slope meant the response was dropping more quickly across repeated startle probes.
Trait Anxiety Was Linked to Weaker Eye-Blink Habituation
Before ultrasound, the clearest anxiety link appeared in the EMG startle measure. Participants with higher trait anxiety scores showed weaker eye-blink habituation in both early and late windows.
The paper reported Spearman correlations of about 0.32 for the early window and 0.37 for the late window. In plain terms, people with higher stable anxiety tended to show flatter reductions in their eye-blink response as the same sound repeated.
That distinction matters because the state-anxiety score taken before each session did not show the same pattern. The finding points more toward a stable trait-linked difference in sensory inhibition than a temporary “I feel anxious today” effect.
The anxiety association also did not generalize across every measure:
- EMG startle: Higher trait anxiety was modestly associated with weaker habituation.
- EEG response: Trait and state anxiety were not reliably linked to habituation slope.
- EDR response: Trait and state anxiety were not reliable predictors before stimulation.
This makes the EMG result useful but bounded. It suggests startle habituation may capture one anxiety-relevant inhibition process, not a universal anxiety signature across all physiological systems.
Focused Ultrasound Improved Early Skin-Conductance Habituation
The main stimulation result was selective. LIFU targeting the anterior insula or anterior midcingulate cortex did not significantly change EMG or EEG habituation compared with sham.
Instead, active ultrasound enhanced early EDR habituation. Skin-conductance responses dropped more quickly after anterior insula or anterior midcingulate stimulation than after sham, indicating a transient improvement in autonomic adaptation to repeated startle sounds.
That is a narrower claim than “focused ultrasound reduced anxiety.” The participants were healthy adults, and the outcome was a short-term physiological response in a lab task. The study does not show clinical symptom improvement or treatment efficacy.
Still, the result gives researchers a causal test point. If salience-network hubs help regulate how the body keeps responding to repeated harmless stimuli, focused ultrasound may offer a way to probe that pathway without surgery or implanted stimulation.
EMG and EEG Moved Together, but EDR Behaved Differently
The cross-signal analysis helps explain why the result should not be flattened into one startle score. EMG and EEG habituation were correlated, with stronger eye-blink habituation generally tracking stronger cortical habituation.
EDR was different. Autonomic habituation did not consistently move with the EMG or EEG measures, which fits the stimulation result: ultrasound changed the autonomic channel without producing a matched shift in the muscle or cortical channels.
That split may be clinically important later. Anxiety involves subjective worry, defensive reflexes, attention, and autonomic arousal, but those systems do not always move together.
A person can show strong physiological arousal even when a reflex or cortical response has already adapted.
For future studies, the practical question is whether this short-term autonomic effect can be reproduced in people with anxiety disorders and whether repeated sessions alter symptoms, avoidance, or threat monitoring. The current experiment is best read as a mechanistic signal, not a ready treatment protocol.
The Result Is Promising but Still Early
The strongest part of the study is its within-person design. Each participant served as their own comparison across anterior insula, anterior midcingulate, and sham sessions, reducing the chance that the result simply reflects differences between people.
The main limitation is also straightforward: 40 healthy participants is not a clinical anxiety trial. The study measured immediate habituation after stimulation, not durable anxiety relief, daily functioning, or treatment response.
Even with that caveat, the paper gives anxiety research a useful target. It separates trait-linked startle inhibition from autonomic habituation and shows that salience-network ultrasound can selectively shift the latter.
If later work confirms the effect in clinical samples, habituation slopes could become a practical physiology readout for testing neuromodulation strategies. For now, the message is narrower and cleaner: focused ultrasound changed one anxiety-relevant autonomic adaptation signal, not the whole startle system.
Citation: DOI: 10.1016/j.bpsgos.2026.100732. Legon et al. Focused ultrasound neuromodulation of salience network hubs selectively enhances anxiety-relevant autonomic habituation in humans. Biological Psychiatry: Global Open Science. 2026;6:100732.
Study Design: Single-blind, sham-controlled crossover human experiment.
Sample Size: 40 healthy adults, including 28 women and 12 men.
Key Statistic: Active anterior insula or anterior midcingulate LIFU enhanced early EDR habituation relative to sham, while EMG and EEG habituation did not significantly change.
Caveat: The result is an immediate laboratory physiology effect in healthy participants, not evidence that LIFU treats anxiety disorders.