TL;DR: A 2026 randomized trial posted to medRxiv found that connectivity-guided accelerated intermittent theta-burst stimulation added to inpatient care improved treatment-resistant depression scores more than sham stimulation over 2 weeks.
Key Findings
- 57 randomized patients: Hospitalized adults with unipolar treatment-resistant depression were assigned to active or sham stimulation.
- 30 iTBS sessions: Active treatment delivered 3 daily sessions across 10 weekdays, totaling 54,000 pulses.
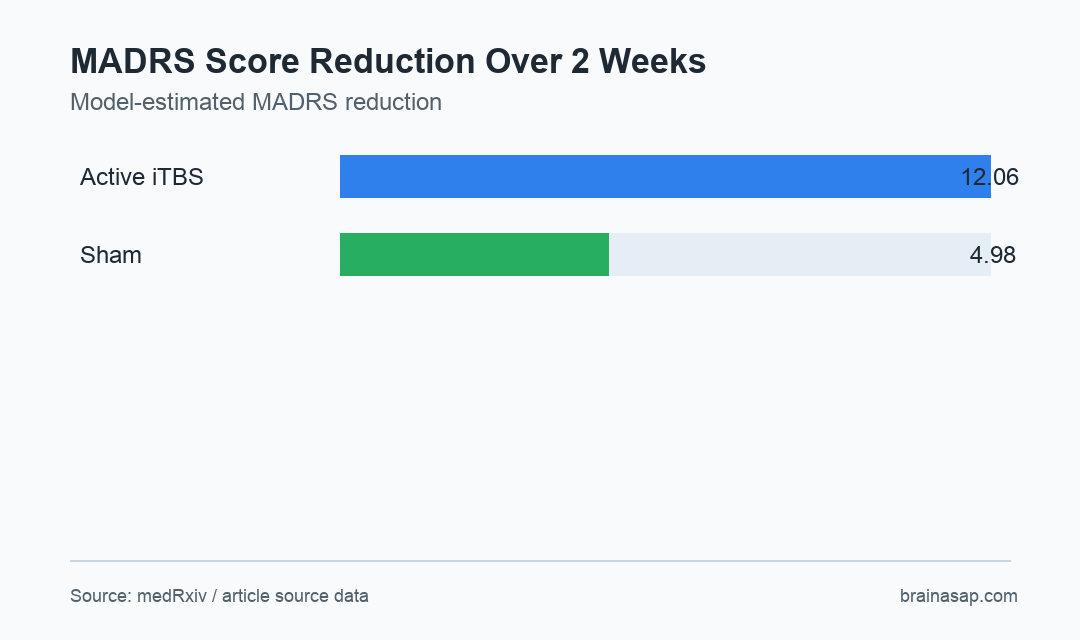
- 12.06 vs 4.98 points: Model-estimated MADRS depression-score reduction was larger with active iTBS than sham.
- 42.3% response: MADRS response occurred in 42.3% of active-treatment patients versus 13.0% with sham.
- No serious adverse events: The acute inpatient protocol reported no serious adverse events during the stimulation phase.
Source: medRxiv (2026) | Kaur et al.
Treatment-resistant depression often requires more than one medication or therapy approach, especially when symptoms are severe enough for inpatient care. Intermittent theta-burst stimulation, or iTBS, is a patterned magnetic stimulation method that can target cortical circuits involved in mood regulation.
This trial tested a more individualized version. Resting-state functional MRI identified a left dorsolateral prefrontal cortex target that was most anticorrelated with the subgenual anterior cingulate cortex, a depression-relevant region often shortened as sgACC.
Connectivity-Guided iTBS Targeted a Personalized Depression Circuit
The trial enrolled hospitalized patients with unipolar depression and moderate-to-severe treatment resistance. Of 57 randomized patients, 51 completed the stimulation phase: 27 in the active group and 24 in the sham group.
Active stimulation was not a single-session intervention. Patients received 3 sessions per day over 10 weekdays, producing 30 sessions and 54,000 pulses during a 2-week inpatient augmentation period.
- Targeting method: Functional MRI selected a patient-specific left dorsolateral prefrontal cortex site anticorrelated with sgACC.
- Clinical setting: Stimulation was added to routine multimodal inpatient care rather than tested as a stand-alone outpatient intervention.
- Primary outcomes: Depression change was measured with the Montgomery-Asberg Depression Rating Scale (MADRS) and Beck Depression Inventory-II (BDI-II).
- Blinding: The design was randomized, double-blind, and sham-controlled, which helps reduce expectancy bias.
The design makes the result clinically relevant for a difficult group, but it also narrows interpretation. The trial tested inpatient add-on treatment, not whether iTBS alone replaces medication, psychotherapy, or hospital-based care.
The trial population also had substantial illness burden. The source described moderate-to-severe treatment resistance, with mean Maudsley Staging Method score 10.9, plus high psychiatric comorbidity.
That context helps explain why a sham-controlled inpatient design is valuable. Symptom change during hospitalization can reflect many simultaneous supports, so the sham arm is essential for estimating the added stimulation effect.
MADRS Improvement Favored Active iTBS Over Sham
MADRS scores improved faster in the active-treatment group. The group-by-time estimate favored active iTBS by -3.54 points per week, with a 95% confidence interval from -5.53 to -1.55 after false-discovery-rate correction.
Model estimates translated that slope into a larger 2-week reduction: 12.06 MADRS points for active iTBS versus 4.98 points for sham. The reported effect size for MADRS change was large, with d=-0.89.
The self-report BDI-II trajectory also favored active treatment, though the effect was smaller. The group-by-time estimate was -0.23 points per day, with a 95% confidence interval from -0.41 to -0.05.
- Clinician-rated change: MADRS improvement was the clearest efficacy result.
- Self-reported symptoms: BDI-II change moved in the same direction but with a smaller effect.
- Acute time window: Outcomes covered the 2-week stimulation phase, so durability remains unresolved.
Response Rates Increased More Clearly Than Remission Rates
Response rates also favored active stimulation. MADRS response occurred in 42.3% of active iTBS patients compared with 13.0% in the sham group.
Remission was numerically higher with active treatment, at 26.9% versus 12.5%, but that difference was not statistically significant in the reported exploratory endpoints. That split is important: symptom reduction was clearer than confirmed remission.
- Strongest clinical result: Faster and larger MADRS score reduction during acute treatment.
- Supportive response result: Higher response rate with active stimulation.
- Less certain remission result: Remission difference was numerically favorable but not significant.
- Safety finding: No serious adverse events were reported during the trial period.
The absence of serious adverse events is reassuring for feasibility, especially because the protocol delivered repeated daily sessions. It does not remove the need for larger safety datasets, longer follow-up, or real-world implementation checks.
The response-remission split is also clinically familiar. A patient can improve enough to meet response criteria while still having meaningful residual symptoms, so remission and relapse prevention deserve their own follow-up endpoints.
Larger Multicenter Trials Need to Test Durability and Workflow
The study supports connectivity-guided accelerated iTBS as a promising inpatient augmentation strategy. It does not establish how long the benefit lasts, whether booster sessions are needed, or whether the same workflow scales outside a specialized setting.
Personalized targeting also carries a practical requirement: patients need MRI-based connectivity mapping before treatment. That may improve biological precision, but it adds cost, scheduling complexity, and technical demands compared with simpler stimulation protocols.
The protocol may be best suited first for centers that already have neuroimaging, stimulation expertise, and inpatient mood-disorder workflows. Broader use would require simpler scheduling and clear rules for who benefits most.
The next evidence step is a larger multicenter trial with longer follow-up and prespecified remission, relapse, and functioning outcomes. For now, the trial gives a concrete finding: connectivity-guided iTBS improved acute depression scores beyond sham in a severely ill inpatient sample.
Citation: DOI: 10.64898/2026.06.25.26356553. Kaur et al. Connectivity-guided accelerated theta burst stimulation as augmentation for inpatient treatment-resistant depression: a randomized, double-blind, sham-controlled trial. medRxiv. 2026.
Study Design: Randomized, double-blind, sham-controlled inpatient augmentation trial.
Sample Size: 57 randomized patients with unipolar treatment-resistant depression; 51 completed treatment.
Key Statistic: Model-estimated MADRS reduction was 12.06 points with active iTBS versus 4.98 points with sham.
Caveat: The source is a preprint with short acute follow-up, so durability and broader implementation remain open questions.