TL;DR: A 2026 protocol posted to medRxiv describes a nationwide Japan survey designed to measure how dementia specialists handle anti-amyloid antibody therapy, biomarker testing, MRI safety monitoring, service capacity, and patient-choice tradeoffs.
Key Findings
- Nationwide specialist survey: The protocol targets board-certified dementia specialists in Japan, especially physicians trained for anti-amyloid antibody therapy.
- June 2026 data collection: Survey collection started June 3, 2026 and was planned to close June 30, 2026.
- Two preference methods: The design includes a discrete choice experiment and best-worst scaling.
- Six treatment attributes: Hypothetical therapy profiles vary by efficacy, ARIA risk, treatment duration, visit frequency, waiting time, and monthly out-of-pocket cost.
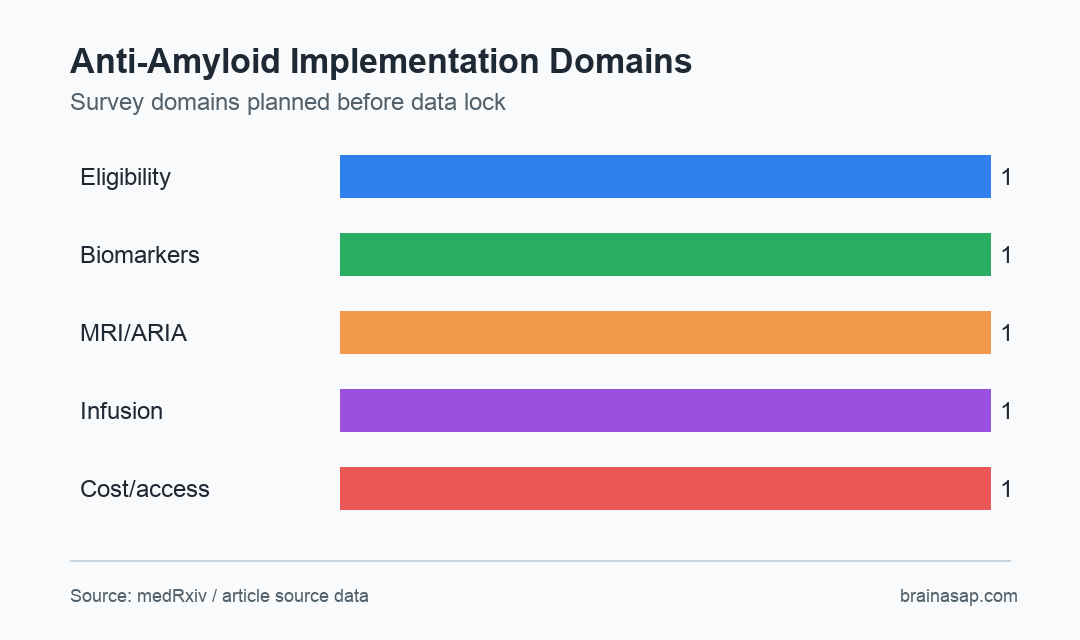
- Pre-data-lock protocol: The manuscript was prepared before outcome analyses, so it reports survey design rather than final survey results.
Source: medRxiv (2026) | Sato et al.
Anti-amyloid antibody therapies such as lecanemab and donanemab have changed early Alzheimer disease care. They also require biomarker confirmation, repeated MRI scans, infusion logistics, safety monitoring, and careful shared decision-making.
This protocol focuses on Japan’s real-world implementation problem. Under universal public health insurance and optimal use guidelines, access depends not only on drug approval but also on whether facilities can deliver diagnosis, monitoring, and treatment safely.
Japan Survey Targets Dementia Specialists Managing Anti-Amyloid Therapy
The planned survey is a prospective, cross-sectional, anonymous online survey using Google Forms. It targets board-certified specialists of the Japanese Society for Dementia Research and the Japanese Psychogeriatric Society.
The main focus is physicians who completed the official training course required for anti-amyloid antibody therapy. The survey therefore centers on clinicians facing the treatment workflow, not general opinion.
- Respondent profile: Specialist background, facility characteristics, and treatment experience.
- Diagnostic workflow: Eligibility assessment, amyloid testing, APOE testing, and blood-based biomarker views.
- Safety workflow: MRI monitoring and amyloid-related imaging abnormality management.
- Service workflow: Infusion capacity, continued-administration facilities, waiting time, and reimbursement barriers.
Because the source is a protocol, it does not report whether Japanese dementia specialists view one barrier as dominant. It tells readers what the study planned to measure before data lock.
The timing also matters. Data collection began on June 3, 2026 and was planned to close on June 30, 2026, so the protocol was published around the active survey window rather than after results were known.
That helps protect interpretability. A public analysis plan makes it harder to choose only favorable or surprising findings after responses arrive.
Discrete Choice Experiment Tests Therapy Tradeoffs
The discrete choice experiment asks respondents to choose between hypothetical anti-amyloid antibody treatment profiles for early Alzheimer disease. Each profile varies by expected benefit, risk, burden, access delay, and patient cost.
The design is useful because these drugs are not judged on efficacy alone. A therapy with modest slowing of decline may look different if MRI monitoring is frequent, treatment lasts longer, ARIA risk is higher, or monthly out-of-pocket cost changes.
- Expected efficacy: How much benefit specialists assume the profile provides.
- ARIA risk: Risk of amyloid-related imaging abnormalities requiring interruption or discontinuation.
- Treatment burden: Treatment duration and visit frequency.
- Access burden: Waiting time and monthly out-of-pocket cost.
Best-worst scaling adds a policy lens by asking which system-level solutions are most and least important. That can separate clinical treatment preference from infrastructure priorities.
Cost is part of the design because Japan’s public insurance system still leaves practical patient-facing decisions. Even when a therapy is covered, visit frequency, time off work, caregiver support, and regional travel can change willingness to proceed.
Blood Biomarkers and MRI Monitoring Sit Inside the Same Care Pathway
Blood-based biomarkers could help triage who needs more expensive or invasive Alzheimer disease testing. The protocol asks specialists how these tests might fit into routine care, especially as amyloid and tau blood assays move closer to clinical use.
Safety monitoring remains separate. Anti-amyloid antibodies can cause amyloid-related imaging abnormalities, so MRI access and interpretation are not optional details.
A facility can support the drug and still lack the workflow to monitor it well.
- Biomarker bottleneck: Amyloid confirmation and emerging blood tests affect who enters the treatment pathway.
- Imaging bottleneck: Repeated MRI monitoring affects safety, capacity, and patient burden.
- Infusion bottleneck: Treatment delivery depends on staff, space, scheduling, and continuation sites.
- Policy bottleneck: Reimbursement and regional coordination shape whether guidelines become practical care.
The protocol’s strength is that it treats Alzheimer antibody treatment as a system. Drug efficacy is only one part of whether patients can actually be evaluated, started, monitored, and continued.
APOE testing is another example of that system problem. APOE genotype can affect ARIA risk discussions, but adding genetic testing changes counseling, consent, privacy, and appointment flow.
Protocol Results Will Need Careful Interpretation After Data Lock
Since this is a pre-results protocol, no outcome claims should be inferred. The survey may identify major barriers, but the direction and size of those barriers were not available in the source.
Online specialist surveys can also be affected by response bias. Physicians with strong opinions or direct treatment experience may be more likely to respond, and facility-level capacity may vary by region in ways that a survey must describe carefully.
The operational takeaway is direct: anti-amyloid antibody implementation depends on trained specialists, biomarker access, MRI safety pathways, infusion capacity, patient preferences, and reimbursement. The final survey findings should be read against that prespecified structure.
Citation: DOI: 10.64898/2026.06.30.26356494. Sato et al. Protocol for the 2026 Nationwide Survey of Dementia Specialists on the Real-World Implementation of Anti-Amyloid Antibody Therapies in Japan: Clinical Practice, Blood Biomarkers, and Preference Experiments. medRxiv. 2026.
Study Design: Prospective cross-sectional anonymous online survey protocol with discrete choice experiment and best-worst scaling components.
Sample Size: Survey sample size was not reported in the source excerpt; data collection was planned among Japanese dementia specialists.
Key Statistic: The discrete choice experiment varies six treatment attributes: efficacy, ARIA risk, duration, visit frequency, waiting time, and monthly out-of-pocket cost.
Caveat: This protocol was prepared before data lock and does not report final survey findings.