TL;DR: A 2026 pilot randomized trial in Nursing in Critical Care found that an 8-week home-based program combining exercise with computerized cognitive training was feasible in 36 ICU survivors and produced larger reductions in patient-reported post-intensive care syndrome severity than attention control, while exploratory cognitive and quality-of-life effect sizes generally favored the combined program over exercise alone.
Key Findings
- 36 ICU survivors: Researchers randomized 13 people to COMBAT-ICU, 12 to exercise-only rehabilitation, and 11 to attention control.
- 8-week home program: COMBAT-ICU combined progressive exercise with computerized cognitive training across 3 sessions per week.
- High adherence: COMBAT-ICU participants completed 285 of 312 planned sessions, for a 91.3% session adherence rate.
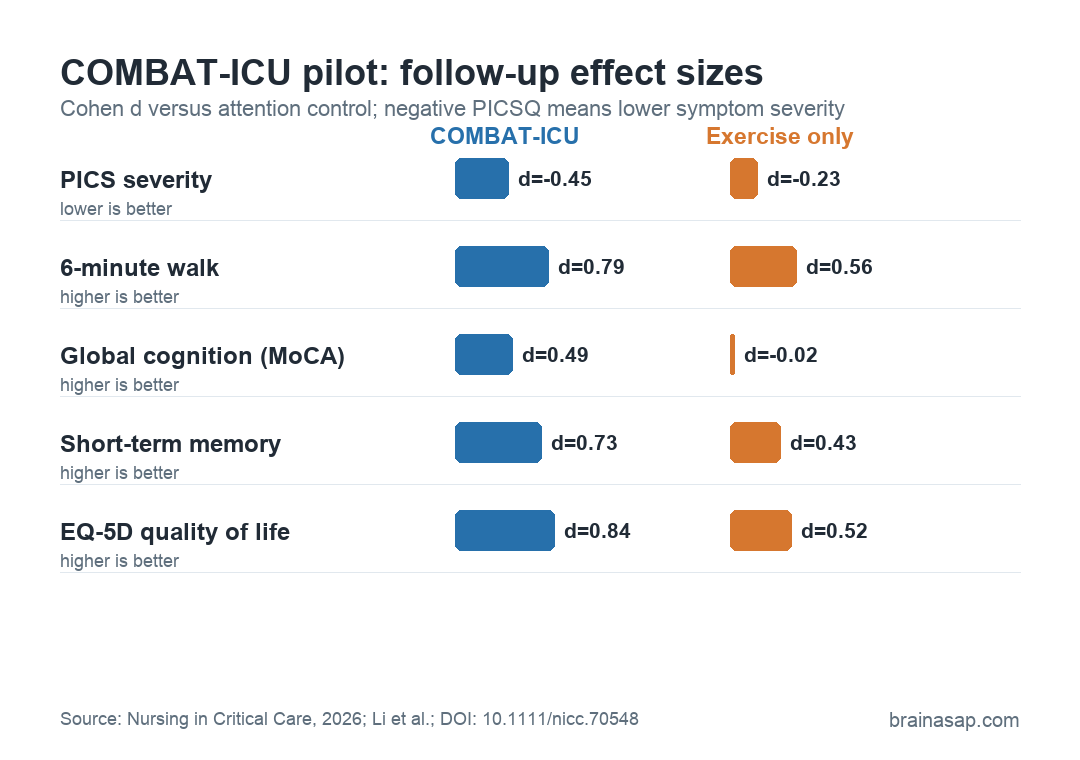
- PICS severity fell: COMBAT-ICU reduced PICS severity more than attention control after treatment (p = 0.014, d = -0.50) and at 3-month follow-up (p = 0.043, d = -0.45).
- Cognitive results favored combined training: Global cognition, attention/processing speed, short-term memory, and quality-of-life effect sizes generally favored COMBAT-ICU over exercise alone.
Source: Nursing in Critical Care (2026) | Li et al.
Post-intensive care syndrome is the long recovery problem that can follow survival from critical illness. It can include physical weakness, cognitive problems, anxiety, depression, reduced daily function, and lower quality of life after an ICU stay.
This trial tested whether rehabilitation should address those domains together instead of treating physical recovery as the whole problem. The intervention, called COMBAT-ICU, paired home-based progressive exercise with computerized cognitive training for ICU survivors judged to be at risk of post-intensive care syndrome.
COMBAT-ICU Combined Exercise With Cognitive Training
The study was a three-arm, assessor-blinded pilot randomized controlled trial conducted in Hong Kong. Researchers enrolled 36 ICU survivors who had spent at least 4 days in the ICU, were returning home, had family support, and could walk at least 10 meters with or without help.
Participants were randomized to one of three groups:
- COMBAT-ICU: An 8-week combined program with 45 minutes of exercise, a 5-minute break, and 30 minutes of cognitive training per session.
- Exercise-only rehabilitation: The same progressive home-based exercise structure without the computerized cognitive component.
- Attention control: Health-monitoring contact designed to match attention without delivering the active physical or cognitive training.
The exercise portion targeted mobility, balance, strength, and endurance. Delivery shifted by functional level, using supervised home visits, real-time online sessions, and later self-directed practice when participants were ready.
The cognitive portion used computerized training focused on attention, memory, and executive function. Many ICU survivors do not have only a strength problem.
Memory, attention, mental fatigue, and daily planning can all remain impaired after discharge.
PICS Severity Improved More Than Attention Control
The strongest symptom result came from the Post-Intensive Care Syndrome Questionnaire (PICSQ), an 18-item patient-reported measure of PICS severity. COMBAT-ICU showed larger PICSQ improvement than attention control immediately after the intervention and at follow-up.
At the post-intervention assessment, the COMBAT-ICU versus attention-control comparison showed p = 0.014 and Cohen’s d = -0.50.
At the 3-month follow-up, the comparison remained statistically significant, with p = 0.043 and d = -0.45. The negative effect size means lower reported PICS severity.
Exercise-only rehabilitation moved in the same direction, but the effect sizes were smaller: d = -0.29 after treatment and d = -0.23 at follow-up.
The comparison does not prove that the cognitive training component caused the entire difference. The trial was small and exploratory.
It does show that the combined program produced the more consistent PICS-severity result in this pilot sample.
Physical Recovery Improved in Both Active Groups
Walking endurance improved in both active rehabilitation groups. On the 6-minute walk test, COMBAT-ICU had a large effect versus attention control after treatment (d = 0.93), while exercise-only rehabilitation was very similar (d = 0.89).
By 3 months, the walking effect attenuated but still favored both active groups. COMBAT-ICU showed d = 0.79, while exercise-only showed d = 0.56.
Lower-extremity function, measured by the Short Physical Performance Battery, showed smaller effects after treatment and medium-size estimates for COMBAT-ICU at follow-up.
The physical-function result is not a null finding for exercise alone. Physical training appeared to help physical function.
Some recovery likely also reflected the natural improvement many ICU survivors experience during the first months after discharge.
Cognitive and Quality-of-Life Results Favored Combined Training
The cognitive results were exploratory, but they favored the combined program more than the exercise-only program.
For Montreal Cognitive Assessment (MoCA) scores, COMBAT-ICU showed a small effect after treatment (d = 0.26) that increased to d = 0.49 at follow-up. Exercise-only effects were negligible.
Attention and processing speed, measured with Colour Trails Test 1, also favored COMBAT-ICU. The effect sizes were d = -0.45 after treatment and d = -0.60 at follow-up, where lower completion time indicates better performance.
- Short-term memory: Digit span forward showed medium effects for COMBAT-ICU at both time points, including d = 0.73 at follow-up.
- Higher-order executive function: Colour Trails Test 2 and digit span backward showed smaller or negligible effects.
- Mental health: Anxiety and depression effects were small across active groups, so the program should not be read as a strong anxiety or depression intervention from this pilot.
- Quality of life: EQ-5D index scores favored COMBAT-ICU at follow-up, with a large effect-size estimate of d = 0.84.
These results fit the study’s practical logic. A combined motor-cognitive intervention may be most useful when the recovery problem itself is multidomain.
Feasibility Was the Main Pilot-Trial Result
The feasibility data are central to the trial. The COMBAT-ICU group had 100% completion at both follow-up assessments and completed 91.3% of planned sessions.
No serious adverse events were attributed to the intervention.
Post-ICU rehabilitation often fails at delivery. Patients may have limited mobility, transportation barriers, fatigue, caregiver constraints, and uneven access to clinic-based programs.
A blended home model can reduce some of those barriers while still providing supervision early in recovery.
The authors calculated that a future definitive trial would need 196 randomized participants, allowing for attrition, to test the PICS-severity result with adequate power. That larger trial would also need broader inclusion criteria and longer follow-up.
A Larger COMBAT-ICU Trial Would Need 196 Participants
This was a pilot study, not a definitive proof that COMBAT-ICU should become standard post-ICU care. The sample was small, the confidence intervals were wide, and the 3-month follow-up cannot show whether benefits last through longer recovery.
The eligibility rules also narrowed the population. Participants needed internet access, family support, and enough physical capacity to walk at least 10 meters.
The model still needs testing in more socially isolated survivors, people with fewer digital resources, and patients with heavier neurologic disability.
A narrow conclusion is stronger: a home-based combined exercise and cognitive training program was deliverable after ICU discharge.
It had high adherence and produced enough physical, cognitive, and quality-of-life results to justify a larger multicenter trial.
Citation: DOI: 10.1111/nicc.70548. Li et al. Home-Based Combined Activity and Cognitive Intervention for Post-Intensive Care Syndrome: A Pilot Randomised Controlled Trial. Nursing in Critical Care. 2026;31:e70548.
Study Design: Parallel, three-arm, assessor-blinded pilot randomized controlled trial.
Sample Size: 36 ICU survivors randomized to COMBAT-ICU, exercise-only rehabilitation, or attention control.
Key Statistic: COMBAT-ICU reduced PICS severity versus attention control after treatment (p = 0.014, d = -0.50) and at 3-month follow-up (p = 0.043, d = -0.45).
Caveat: Small feasibility trial with short follow-up and eligibility rules requiring internet access and family support.