TL;DR: A 2026 study in Communications Medicine reported that artificial intelligence (AI) and multi-contrast MRI post-processing could reveal cortical lesions in multiple sclerosis trial scans that standard MRI review usually misses.
Key Findings
- 80-person methods subset: Researchers analyzed 80 people with primary progressive multiple sclerosis from the phase 3 ORATORIO trial, then trained additional models on the full 732-person trial imaging set.
- 1,182 cortical lesions: Multi-contrast review found 1,182 baseline cortical lesions in the 80-person subset, averaging 14.8 lesions per participant.
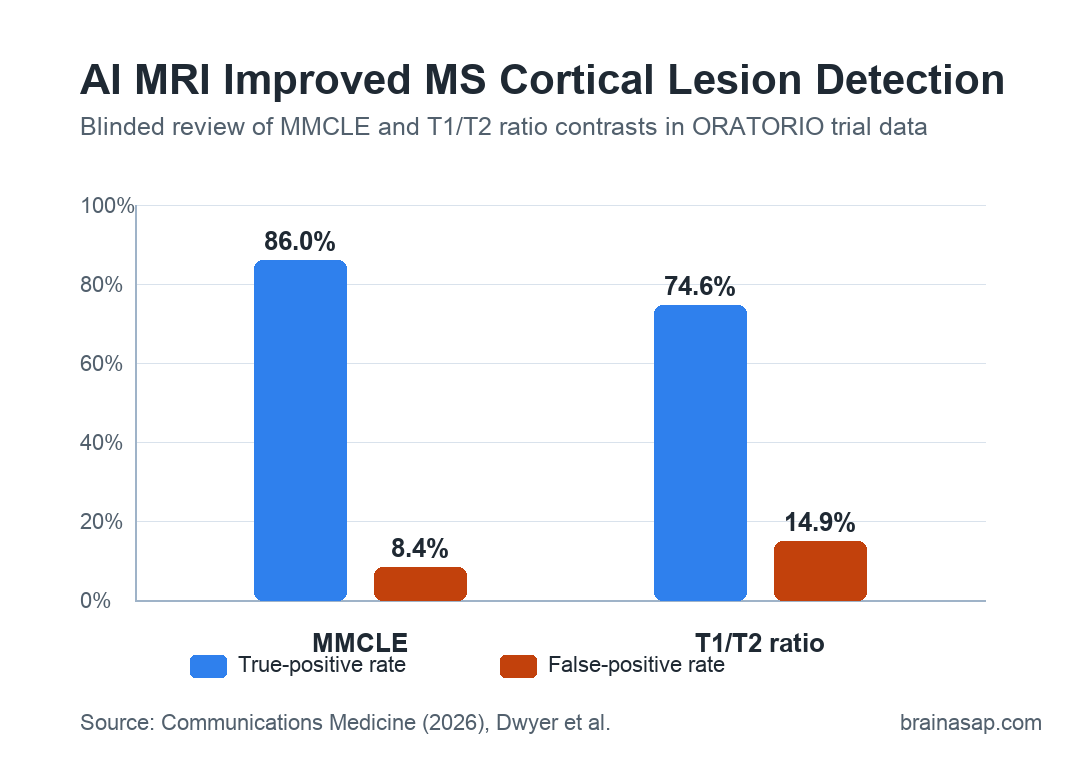
- 86.0% true-positive rate: The multi-modal cortical-lesion enhanced (MMCLE) contrast had the highest blinded-review true-positive rate among individual contrasts.
- 8.4% false-positive rate: MMCLE produced fewer false positives than the T1/T2 ratio contrast, which averaged 14.9% false positives.
- 88.8%-92.5% reproducibility: Additional scanner comparisons showed high agreement for cortical-lesion volume and count across field strength and acquisition differences.
Source: Communications Medicine (2026) | Dwyer et al.
Multiple sclerosis (MS) is often tracked by white-matter lesions, but cortical gray matter damage is also tied to disability, cognition, and disease progression.
The practical problem is visibility. Cortical lesions can be hard to see on conventional 1.5 T or 3 T MRI scans, and 7 T MRI is not realistic for most large trials or routine clinics.
Researchers tested whether already collected clinical-trial MRI scans could be reprocessed to expose more hidden cortical-lesion burden.
The ORATORIO trial already contains high-quality, multicenter imaging from people with primary progressive MS, but those scans were not originally designed around cortical-lesion detection.
AI and Multi-Contrast MRI Reprocessed ORATORIO Trial Scans
Researchers started with an 80-person development subset from the 732-person ORATORIO trial of ocrelizumab in primary progressive MS.
The subset was selected across deciles of total T2 lesion volume so the methods would face a range of lesion burdens rather than an unusually easy group.
The team compared several ways to make conventional MRI data more informative for cortical lesions:
- FLAIR squared: A multiplication-based image contrast built from fluid-attenuated inversion recovery (FLAIR) and T2 images to increase lesion visibility.
- T1/T2 ratio: A ratio image intended to make tissue differences clearer after image alignment and intensity standardization.
- AI-DIR: An artificial intelligence-derived double inversion recovery image generated from standard MRI contrasts.
- MMCLE: A combined contrast that multiplied AI-DIR with FLAIR squared to emphasize areas where both methods pointed to the same abnormal tissue.
The main reference standard was conservative. A lesion had to be visible on multiple contrasts, and at least one confirming contrast had to be non-AI, either FLAIR squared or the T1/T2 ratio.
The confirmation rule was meant to reduce the risk that the AI-derived image would create a lesion-like artifact.
MMCLE Detected More MS Cortical Lesions Than Single Contrasts
At baseline, the combined review identified 1,182 cortical lesions in the 80-person subset, or a mean of 14.8 lesions per participant.
When researchers later applied final training procedures to the full 732-person trial set, they identified 10,366 cortical lesions and 193 new or enlarging cortical lesions.
The clearest individual contrast was MMCLE, short for multi-modal cortical-lesion enhanced. In blinded review, raters correctly identified 86.0% of lesions on MMCLE, compared with 74.6% on the T1/T2 ratio contrast.
False positives also favored MMCLE. The false-positive rate averaged 8.4% for MMCLE, versus 14.9% for T1/T2 ratio.
A useful clinical-trial method has to find subtle lesions without turning every ambiguous cortical intensity change into a lesion call.
Contrast-to-noise results pointed in the same direction. MMCLE had the highest contrast-to-noise ratio when lesions were compared with normal-appearing brain tissue, normal-appearing gray matter, and normal-appearing white matter.
Deep Learning Segmentation Helped Quantify Lesion Burden
After human review, researchers trained transformer-based segmentation models to detect and outline cortical lesions. They used Swin-UNETR, a medical-image segmentation architecture that combines convolutional image features with transformer-style attention.
The AI work had two different jobs:
- Compare input contrasts: Models were trained on each contrast and on contrast combinations to see which images contained the strongest lesion information.
- Build a deployable model: Additional models were trained on the full 732-person imaging set for future analyses of lesion burden and lesion evolution.
- Support longitudinal review: A separate model used paired timepoints to help classify new and enlarging cortical lesions.
Using all four synthetic contrasts improved AI detectability compared with conventional imaging.
The multi-contrast approach improved AI detectability by 1.62-fold over conventional MRI, while MMCLE alone improved AI detectability by 32% compared with conventional imaging.
Standard MRI still is not a perfect cortical-lesion test. Information already present across routine contrasts can be recombined and segmented so cortical lesions become more measurable than they were during ordinary trial review.
Scanner Checks Supported Reproducible Cortical-Lesion Counts
A key question for any retrospective trial method is whether it survives scanner variation. ORATORIO used many scanners across trial sites, and the study also ran supplementary comparisons across field strength and acquisition type.
The stability checks were encouraging:
- Field strength: In 99 people scanned at both 1.5 T and 3 T within one month, cortical-lesion count agreement reached an ICC of 92.5%.
- Lesion volume: The same field-strength comparison showed an ICC of 88.8% for cortical-lesion volume.
- FLAIR acquisition: In 38 people scanned with both 2D and 3D FLAIR at 3 T, count and volume ICC values were 86.2% and 87.2%.
Intraclass correlation coefficient (ICC) is an agreement measure, so these values suggest the pipeline was not simply working on one narrow scanner setup.
This helps if older clinical trials are going to be reanalyzed across sites, vendors, and acquisition protocols.
Subpial MS Lesions Remain the Hardest Boundary
The main limitation is anatomical, not just computational. Cortical lesions come in different forms, and subpial lesions are especially difficult for in vivo MRI, even with advanced methods.
The study found that 75%-82% of visible lesions were leukocortical, meaning the pipeline likely undercounts subpial disease.
Several limits should shape the interpretation:
- Conservative confirmation: Requiring non-AI confirmation likely reduced false positives but may have excluded lesions visible mainly on AI-DIR.
- Macroscopic focus: The method captures cortical lesions visible on 1.5 T and 3 T MRI, not the full microscopic burden of cortical demyelination.
- Treatment effects pending: This analysis established methodology; it did not yet test how ocrelizumab or other MS therapies changed cortical-lesion activity.
The practical result is still substantial. If these methods hold up in additional datasets, researchers could revisit completed MS trials and ask whether treatments affected cortical gray matter pathology, not only conventional white-matter MRI outcomes.
Citation: DOI: 10.1038/s43856-026-01683-7. Dwyer et al. Quantifying cortical lesions in multiple sclerosis MRI datasets using multi-contrast post-processing and deep learning. Communications Medicine. 2026;6:365.
Study Design: Retrospective methods analysis of ORATORIO trial MRI data with multi-contrast post-processing, blinded image review, and deep-learning segmentation.
Sample Size: 80-person development subset from a 732-person primary progressive MS trial; additional training and longitudinal models used the full trial imaging set.
Key Statistic: MMCLE produced an 86.0% true-positive rate and 8.4% false-positive rate in blinded lesion review.
Caveat: The pipeline likely underestimates subpial cortical lesions and has not yet been used here to test treatment effects.