TL;DR: A 2026 narrative review in International Journal of General Medicine argued that apathy in Alzheimer’s disease is tied to damage across motivation circuits, including the anterior cingulate cortex, orbitofrontal cortex, striatum, locus coeruleus, and large-scale brain networks.
Key Findings
- Apathy was framed as its own syndrome: The review separates reduced goal-directed behavior from depression, fatigue, anhedonia, and general cognitive decline.
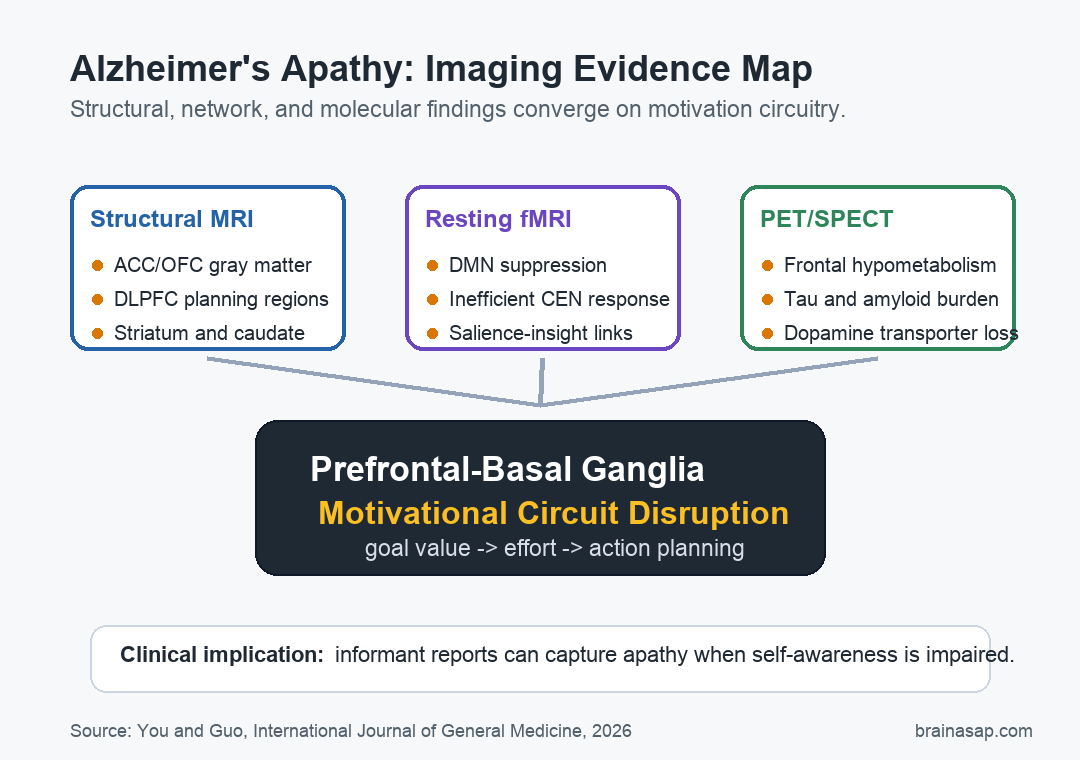
- Motivational circuitry was central: The strongest recurring pattern involved the anterior cingulate cortex, orbitofrontal cortex, dorsolateral prefrontal cortex, and striatum.
- Network findings pointed beyond atrophy: Resting-state fMRI studies linked apathy to default mode network suppression and inefficient central executive network compensation.
- PET studies added molecular context: Tau, amyloid-beta, glucose metabolism, and dopamine transporter findings all pointed toward disrupted motivation and reward signaling.
- Clinical measurement remains limited: Informant reports may track pathology better than patient self-reports when Alzheimer’s disease also impairs insight.
Alzheimer’s apathy is easy to misread as sadness, stubbornness, or ordinary withdrawal. The review makes a narrower claim: in many patients, apathy reflects a breakdown in the brain systems that turn goals, reward value, effort, and action planning into behavior.
That distinction matters because apathy is one of the most common neuropsychiatric symptoms in Alzheimer’s disease. It adds caregiver burden, tracks with worse function, and can appear when a patient does not fully recognize the loss of motivation.
Motivational Circuits Carried the Main Imaging Pattern
The review centers on the prefrontal-basal ganglia motivational circuit. This circuit includes cortical regions that help evaluate reward and plan action, plus subcortical regions that help convert motivation into behavior.
Several nodes came up repeatedly:
- Anterior cingulate cortex: A region involved in motivation, effort, and action selection.
- Orbitofrontal cortex: A region involved in estimating reward value and updating behavior when incentives change.
- Dorsolateral prefrontal cortex: A planning and executive-control region that may matter most for cognitive apathy.
- Striatum and caudate: Subcortical structures that help translate motivational signals into action.
Across structural MRI studies, apathy was linked to gray matter loss in frontal and subcortical motivation regions rather than only to diffuse whole-brain shrinkage. That does not prove these changes cause apathy, but it makes the symptom biologically specific enough to study with imaging.
White matter findings add another layer. Diffusion imaging studies linked apathy with damage in pathways such as the uncinate fasciculus, which connects orbitofrontal and temporal regions involved in emotion, memory, and reward evaluation.
Network Studies Suggested Suppressed Drive and Inefficient Compensation
Structural damage is only part of the picture. Resting-state fMRI studies ask how brain regions communicate when a person is not doing an explicit task. In the review, apathy was tied to altered connectivity within and between major networks.
The default mode network, a system involved in self-referential thought and internally generated behavior, was described as functionally suppressed across Alzheimer’s disease and especially relevant when its midline hubs were affected.
The central executive network showed a different pattern. Some studies reported stronger connectivity in frontal and parietal regions, but the review interprets this as inefficient compensation rather than healthy reserve. In plain terms, more network activity did not necessarily mean better motivation.
The salience network result was more specific. Hyperconnectivity inside parts of that network was linked more to agitation than apathy, while salience-basal ganglia connectivity may matter for reduced insight into apathy symptoms.
Molecular Imaging Added Tau, Amyloid, Dopamine, and Arousal Systems
PET and related molecular imaging studies supplied the review’s strongest bridge between Alzheimer’s pathology and apathy symptoms. FDG-PET, which measures glucose metabolism, linked clinically significant apathy with reduced metabolism in anterior cingulate and orbitofrontal regions.
Tau and amyloid-beta findings were also important, but the paper does not reduce apathy to one protein. The review describes apathy as a circuit-level symptom in which Alzheimer’s pathology damages the regions and connections that support motivation.
Three molecular themes stood out:
- Tau burden: Baseline apathy severity was linked to tau in motivational circuits, while progression may track tau spread into additional cortical regions.
- Dopamine signaling: Lower dopamine transporter binding in the caudate was associated with more severe apathy in cited imaging work.
- Locus coeruleus integrity: Brainstem noradrenergic system damage may reduce arousal and contribute to neuropsychiatric symptoms, including apathy.
Those findings help explain why generic dementia care may miss the target. Apathy can involve reward valuation, effort computation, executive planning, arousal, and self-awareness at the same time.
Informant Reports May Be More Useful Than Self-Reports
The review emphasizes a practical measurement problem: some patients with Alzheimer’s disease have anosognosia, or reduced awareness of their own symptoms. If a patient does not notice the motivational change, self-report scales can understate the problem.
That is why informant-based tools such as caregiver reports remain important. The review cites evidence that informant-reported apathy aligned with Alzheimer’s biomarker burden better than patient self-ratings in some studies.
For clinicians and families, this does not mean every quiet day is pathology. It means repeated loss of initiative, reduced goal-directed behavior, and emotional flattening should be described concretely, with examples, rather than dismissed as mood or personality change.
The Evidence Is Mechanistic, Not a Treatment Rule
This review points toward potential treatment targets, including transcranial magnetic stimulation, dopaminergic drugs, and noradrenergic strategies. It does not show that any one intervention reliably treats Alzheimer’s apathy.
The authors are clear about limitations. Much of the imaging evidence is cross-sectional, sample sizes vary, apathy scales differ, and patients are often at different stages of Alzheimer’s disease. Those differences can shift the apparent location or direction of imaging findings.
The useful conclusion is narrower: apathy in Alzheimer’s disease is not just a vague behavioral label. Imaging studies increasingly place it in damaged motivation circuits, disrupted large-scale networks, altered neurotransmitter systems, and Alzheimer’s protein pathology.
Future longitudinal studies need to test whether these markers can predict who develops apathy, whose symptoms worsen, and which circuit profile responds to a targeted intervention. Until then, multimodal imaging is best understood as a mechanistic map, not a standalone clinical test.
Citation: DOI: 10.2147/IJGM.S622802. You and Guo. Multimodal neuroimaging mechanisms of apathy in Alzheimer’s disease: a narrative review of structural, functional, and molecular evidence. International Journal of General Medicine. 2026;19:622802.
Study Design: Narrative review of structural MRI, diffusion imaging, resting-state fMRI, PET/SPECT, and computational modeling evidence.
Sample Size: Not pooled; the review synthesized previously published imaging and behavioral studies through targeted PubMed searches and reference tracking.
Key Statistic: No pooled effect estimate was reported; the central conclusion was convergence on prefrontal-basal ganglia motivational circuit dysfunction.
Caveat: Narrative review methods, cross-sectional source studies, varied apathy scales, and disease-stage heterogeneity limit causal interpretation.