TL;DR: A 2026 preprint on medRxiv found that in-person cognitive behavioral therapy for insomnia and several shorter behavioral versions were linked with higher post-treatment insomnia remission than sleep hygiene or other control conditions, but the evidence was strongest for full CBT-I.
Key Findings
- 77 randomized trials: The network meta-analysis included 77 RCTs with 5,731 adults who had insomnia, with or without comorbidities.
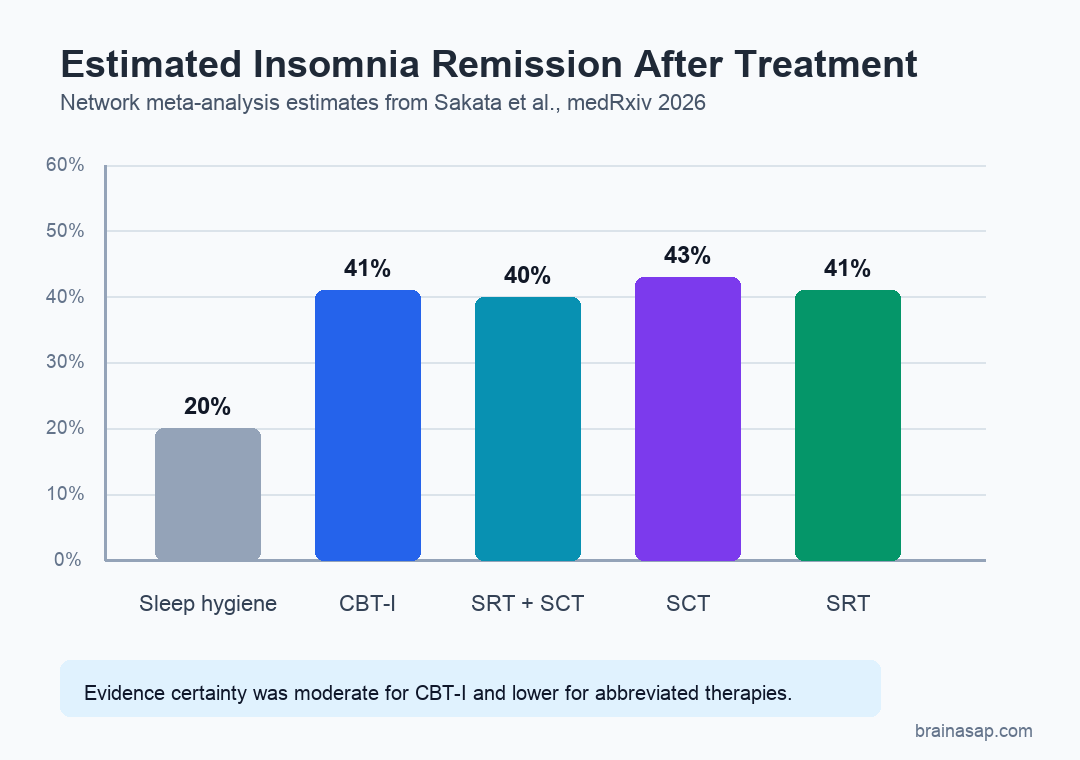
- 41% CBT-I remission: With sleep hygiene remission weighted at 20%, full CBT-I probably led to remission in 41% of patients (95% CI, 34% to 48%).
- 40% combined behavioral remission: Sleep restriction plus stimulus control therapy may have led to 40% remission (95% CI, 30% to 52%).
- Similar dropout: Dropout did not differ meaningfully between active insomnia interventions and control conditions.
- Evidence certainty split: Confidence was moderate for CBT-I, low for sleep restriction combinations, and very low for stimulus control therapy alone.
Source: medRxiv (2026) | Sakata et al.
Cognitive behavioral therapy for insomnia (CBT-I) is a structured psychological treatment that targets the habits, timing, and beliefs that keep insomnia going. The question in this preprint was whether shorter in-person versions of CBT-I could preserve much of the benefit while using fewer clinical resources.
The authors reviewed randomized controlled trials in adults with insomnia and compared full CBT-I, abbreviated behavioral therapies, relaxation therapy, sleep hygiene, and other control conditions in a single network meta-analysis.
CBT-I and Shorter Behavioral Therapies Were Compared Across 77 RCTs
The analysis searched MEDLINE, Embase, PsycINFO, and Cochrane CENTRAL from database inception through December 15, 2025. Screening, extraction, coding, and risk-of-bias assessment were performed independently and in duplicate.
Only in-person randomized controlled trials were included. The restriction reduces delivery-related heterogeneity because digital care, self-help materials, and hybrid formats can differ in adherence, therapist contact, and treatment intensity.
- CBT-I: Full cognitive behavioral therapy for insomnia was represented by 53 arms and 2,002 participants.
- SRT+SCT: Sleep restriction therapy plus stimulus control therapy was represented by 16 arms and 549 participants.
- SRT alone: Sleep restriction therapy was represented by 5 arms and 196 participants.
- SCT alone: Stimulus control therapy was represented by 7 arms and 144 participants.
The primary outcome was insomnia remission after treatment. Secondary outcomes included dropout and subjective sleep-continuity measures, such as patient-reported sleep timing and continuity.
Full CBT-I Probably Doubled Remission Compared With Sleep Hygiene
The anchor comparison was sleep hygiene, which had a weighted mean remission proportion of 20%. Against that reference, full CBT-I probably raised remission to 41%, with a 95% confidence interval from 34% to 48%.
That is the cleanest result in the preprint because the evidence certainty for CBT-I was rated moderate using confidence in network meta-analysis methods. The short version: CBT-I still has the strongest support among the active behavioral options.
- Primary outcome: Remission means moving out of the insomnia-defined state at post-treatment, rather than only showing a small score improvement.
- Control reference: Sleep hygiene was used as the main absolute-rate benchmark in the abstract.
- Clinical interpretation: A 41% versus 20% remission contrast suggests a meaningful treatment advantage, while still leaving many patients symptomatic.
Sleep Restriction and Stimulus Control Looked Similar, With Less Certain Evidence
The abbreviated therapies had remission estimates close to CBT-I. Sleep restriction plus stimulus control therapy may have produced remission in 40% of patients, sleep restriction alone in 41%, and stimulus control alone in 43%.
Those numbers should not be read as proof that the shorter approaches are interchangeable with CBT-I. The confidence intervals were wider, and evidence certainty was lower for the abbreviated arms.
- SRT+SCT estimate: 40% remission, with a 95% confidence interval from 30% to 52%.
- SCT estimate: 43% remission, with a 95% confidence interval from 25% to 63%.
- SRT estimate: 41% remission, with a 95% confidence interval from 26% to 57%.
This is the practical tension in the review. Abbreviated behavioral therapy could help clinics stretch limited behavioral sleep medicine capacity, but implementation decisions have to account for uncertainty, patient fit, therapist training, and the specific components being offered.
Dropout Did Not Meaningfully Separate Active Insomnia Treatments From Controls
Acceptability was assessed through dropout. The abstract reports that dropout did not differ meaningfully between interventions and control conditions.
That acceptability finding is relevant because CBT-I and sleep restriction can ask patients to change routines in demanding ways. A treatment that improves sleep but produces much higher dropout would be harder to scale.
- Benefit side: CBT-I, sleep restriction, and stimulus control were associated with higher remission and better subjective sleep-continuity measures.
- Burden side: The dropout signal did not show a clear acceptability penalty for active treatment.
- Resource side: Shorter behavioral options may be attractive where full CBT-I access is limited, but the evidence grade was lower.
Cognitive therapy for insomnia also appeared more beneficial than relaxation therapy, according to the abstract. The authors noted that CT-I needs more investigation, so it should not be treated as the main implementation answer from this analysis.
Evidence Certainty Favored Full CBT-I Over Abbreviated Versions
The biggest limitation is not that the abbreviated therapies failed. Their evidence was thinner.
Confidence was moderate for CBT-I, low for SRT+SCT and SRT, and very low for SCT.
The source is also a preprint, so the findings have not completed peer review. The included trials were restricted to in-person delivery, which improves comparability but limits direct conclusions about digital CBT-I or app-based insomnia programs.
- Preprint status: The manuscript is available on medRxiv and may change after peer review.
- Delivery scope: The analysis focused on in-person treatment, not digital, app-based, or self-guided care.
- Network assumptions: Indirect comparisons in network meta-analysis depend on how comparable the trial populations and control conditions are.
- Component uncertainty: Similar remission estimates do not prove that every shorter package will work equally well in routine care.
The narrow conclusion is useful for sleep clinics and mental health systems: full CBT-I remains the best-supported behavioral treatment, while shorter in-person behavioral components may offer a reasonable access strategy when resources are limited.
Citation: DOI: 10.64898/2026.07.04.26357278. Sakata et al. Comparative efficacy and acceptability of cognitive-behavioural therapy for insomnia and its abbreviated versions: a systematic review and network meta-analysis. medRxiv. 2026.
Study Design: Systematic review and frequentist random-effects network meta-analysis of in-person randomized controlled trials.
Sample Size: 77 RCTs with 5,731 adults with insomnia.
Key Statistic: CBT-I probably led to 41% remission compared with a 20% weighted remission rate in sleep hygiene arms.
Caveat: The source is a preprint, and evidence certainty was lower for abbreviated behavioral therapies than for full CBT-I.