TL;DR: A 2026 systematic review and meta-analysis in Journal of Medical Internet Research found that immersive virtual reality reduced anxiety and pain in randomized trials of gastrointestinal cancer care, but wide prediction intervals and low evidence certainty mean the effect may vary across clinical settings.
Key Findings
- 14 RCTs: The review included 14 randomized controlled trials with 837 patients with colorectal, liver, esophageal, gastric, pancreatic, or biliary tract cancers.
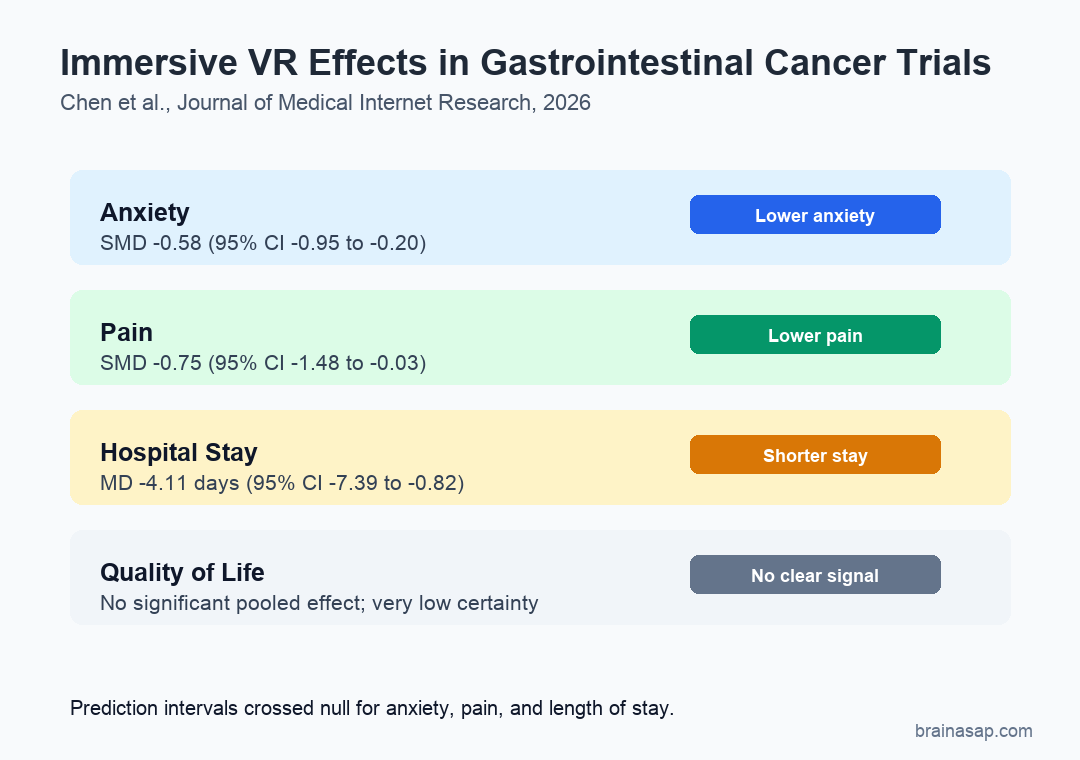
- Anxiety reduction: Immersive virtual reality reduced anxiety versus control conditions (SMD -0.58, 95% CI -0.95 to -0.20; P=.01).
- Pain reduction: The pooled pain result also favored immersive VR (SMD -0.75, 95% CI -1.48 to -0.03; P=.04).
- 4.11 fewer days: Hospital stay was shorter in the VR group by a mean difference of 4.11 days, but the prediction interval was wide.
- No quality-of-life signal: The meta-analysis did not find significant pooled effects for quality of life, knowledge acquisition, or vital signs.
Source: Journal of Medical Internet Research (2026) | Chen et al.
Immersive virtual reality (IVR) uses a headset or similar display to create a strong sense of presence in a simulated environment. In cancer care, that can mean calming nature scenes, interactive games, anatomical education, or guided relaxation during treatment.
This review focused on gastrointestinal cancer because these patients often face both physical pain and treatment-related anxiety. The question was whether IVR helped manage those symptoms in randomized trials.
14 Randomized Trials Tested VR During Gastrointestinal Cancer Care
The authors searched 12 databases and 1 gray-literature source through April 30, 2026. Eligible studies compared IVR with routine care or nonimmersive alternatives in adults with gastrointestinal cancer.
The final evidence base included 837 patients. The cancers included colorectal, liver, esophageal, gastric, pancreatic, and biliary tract cancers.
- Trial design: 12 studies were 2-arm parallel randomized trials, 1 used a 3-arm design, and 1 used a 4-arm design.
- Clinical timing: 7 studies delivered VR before treatment, 4 during treatment, 2 after treatment, and 1 across a longer perioperative period.
- Intervention content: Most studies used immersive scenes, while some used interactive games, anatomical models, videos, or VR-based cognitive behavioral techniques.
- Delivery staff: 11 studies involved physicians and 3 involved nurses.
That range gives the review clinical reach but also makes the intervention pool methodologically uneven. A guided breathing nature scene during a procedure is not the same intervention as a multivisit VR-CBT program during colorectal cancer care.
Immersive VR Reduced Anxiety, Especially During Active Treatment
7 trials with 528 participants contributed to the anxiety meta-analysis. The pooled result favored IVR, with a standardized mean difference of -0.58 and a 95% confidence interval from -0.95 to -0.20.
The subgroup results sharpened the clinical interpretation. Anxiety reduction was larger when VR was delivered during treatment, with an SMD of -0.95, compared with a smaller nonsignificant estimate before treatment.
- During treatment: IVR delivered during active treatment had an anxiety SMD of -0.95 (95% CI -1.32 to -0.46).
- At least 20 minutes: Sessions lasting 20 minutes or longer had an anxiety SMD of -0.95 (95% CI -1.53 to -0.37).
- Operating room setting: Operating-room studies also showed the strongest anxiety signal, with the same SMD estimate of -0.95.
The likely mechanism is attention and emotional regulation. During procedures, an immersive scene can compete with pain, fear, and treatment cues in real time.
Pain Improved on Average, but Heterogeneity Was High
6 trials with 312 participants contributed to the pain analysis. IVR reduced pain compared with control conditions, with an SMD of -0.75 and a 95% confidence interval from -1.48 to -0.03.
The pain result was more fragile than the point estimate alone suggests. Heterogeneity was high, and the paper reported a 95% prediction interval from -2.43 to 0.93, meaning a future similar study could show a large benefit or little effect.
- Acute procedure pain: VR may work best when distraction can directly compete with a painful procedure.
- Chronic cancer pain: Longer-lasting pain may depend on sleep, inflammation, mood, disease burden, and medication context.
- Protocol mismatch: Short single-session VR and multivisit rehabilitation-style VR should not be treated as a uniform therapy.
In pain management terms, IVR is a plausible adjunct. It is not evidence that VR replaces analgesia, procedural anesthesia, psychological care, or oncology symptom management.
Hospital Stay Was Shorter, but Quality-of-Life Effects Were Not Clear
3 studies found a shorter length of stay with IVR, with a mean difference of -4.11 days. The confidence interval was statistically significant, from -7.39 to -0.82 days.
That estimate needs caution because the prediction interval ran from -13.82 to 5.60 days. The pooled average favored VR, but future settings could plausibly show a smaller effect or no reduction.
- Quality of life: The pooled estimate was not significant, and heterogeneity was very high.
- Knowledge: 2 studies favored VR education numerically, but the pooled effect was not statistically significant.
- Vital signs: Systolic blood pressure, diastolic blood pressure, and heart rate did not show clear pooled effects.
- Safety: 4 studies examined safety; 2 found no significant nausea, vomiting, or dizziness differences, and 2 reported no adverse reactions.
Risk of Bias and Low Certainty Keep the VR Result Preliminary
The review’s main limitation is evidence quality. Of the 14 studies, 3 had high overall risk of bias, 8 had some concerns, and only 3 were rated low risk.
GRADE certainty was low for anxiety and pain, moderate for length of stay, and very low for quality of life. The major reasons included risk of bias, inconsistency, and imprecision.
- Average effect: The pooled anxiety and pain estimates favored IVR.
- Future-setting uncertainty: Prediction intervals crossed the null for anxiety, pain, and length of stay.
- Clinical use: IVR is best read as a supportive adjunct for symptom relief, not a stand-alone cancer-care intervention.
The most useful clinical interpretation is narrow: immersive VR may reduce anxiety and pain during gastrointestinal cancer care, especially when delivered during active treatment for at least 20 minutes. Stronger trials are needed to show which patients, settings, and VR protocols produce reliable benefit.
Citation: DOI: 10.2196/86808. Chen et al. Effects of Immersive Virtual Reality Interventions on Symptom Management in Patients With Gastrointestinal Cancer: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Medical Internet Research. 2026;28:e86808.
Study Design: Systematic review and random-effects meta-analysis of randomized controlled trials.
Sample Size: 14 RCTs with 837 adults with gastrointestinal cancer.
Key Statistic: IVR reduced anxiety (SMD -0.58) and pain (SMD -0.75) compared with control conditions.
Caveat: Evidence certainty was low for anxiety and pain, and prediction intervals suggested future effects may vary widely.