TL;DR: A 2026 systematic review and meta-analysis in Archives of Women’s Mental Health linked prenatal active tobacco smoking with higher odds of postpartum depression, while secondhand smoke and electronic nicotine-product estimates were not statistically clear.
Key Findings
- 29-study review: Researchers included 29 studies in the systematic review and 26 studies in the meta-analysis.
- 15% pooled prevalence: Pooled postpartum depression prevalence was 0.15, with a 95% confidence interval from 0.12 to 0.17.
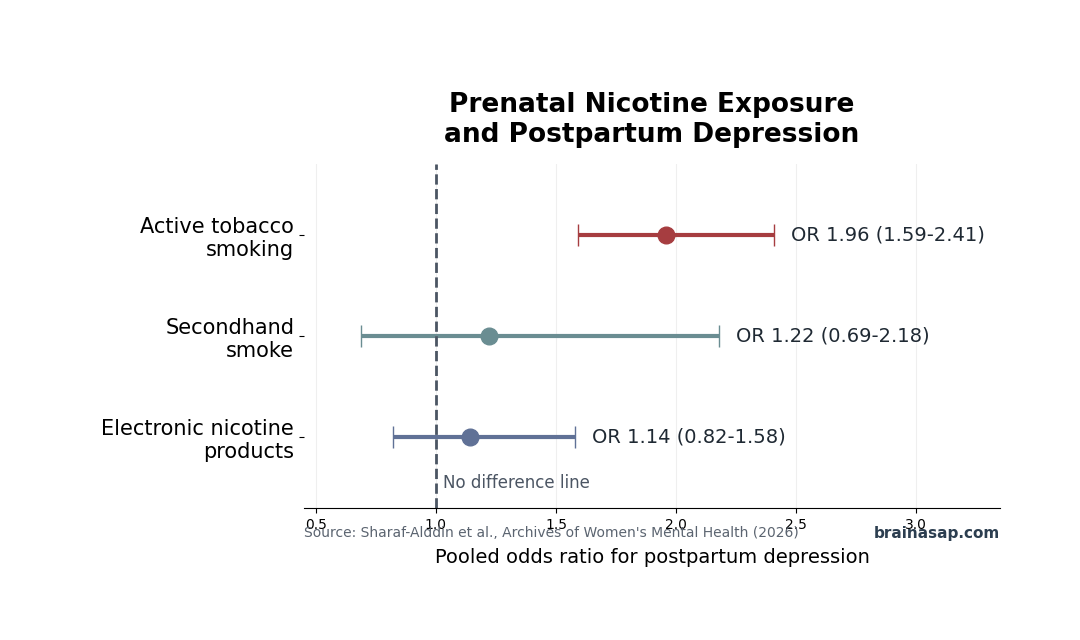
- Active smoking odds: Prenatal active tobacco smoking was associated with higher postpartum depression odds, with a pooled odds ratio of 1.96.
- Secondhand estimate unclear: Prenatal secondhand smoke had a pooled odds ratio of 1.22, but the confidence interval crossed 1.0.
- Electronic nicotine estimate unclear: Electronic nicotine products had a pooled odds ratio of 1.14, also with a confidence interval crossing 1.0.
Source: Archives of Women’s Mental Health (2026) | Sharaf-Alddin et al.
Prenatal nicotine exposure (PEN) is not one exposure in this review. Researchers separated active tobacco smoking, secondhand smoke, and electronic nicotine products because those sources differ in dose, measurement quality, and study volume.
That split is the main reason the paper is more useful than a single pooled nicotine estimate. The broad all-exposure result was positive, but the exposure-specific findings showed that active tobacco smoking carried the strongest and clearest association with postpartum depression.
Active Tobacco Smoking Nearly Doubled Postpartum Depression Odds
The meta-analysis estimated a pooled odds ratio of 1.96 for prenatal active tobacco smoking and postpartum depression. The 95% confidence interval was 1.59 to 2.41, with p < 0.001.
In practical terms, the included studies found higher postpartum depression odds among women who smoked during pregnancy than among comparison groups. Because the evidence is observational, the estimate should be read as an association, not proof that smoking alone caused the depression outcomes.
- Exposure measured: Active tobacco smoking during pregnancy.
- Outcome measured: Postpartum depression, identified through diagnostic tools or screening instruments.
- Main estimate: Pooled odds ratio of 1.96 for active smoking.
- Interpretation limit: Smoking can cluster with stress, socioeconomic risk, prior depression, substance use, and health-care access.
The review still matters clinically because active smoking is a modifiable exposure that is already targeted in prenatal care. A depression-risk signal adds another reason to treat smoking cessation as part of maternal mental health prevention, not only fetal or obstetric risk reduction.
Secondhand Smoke and Electronic Nicotine Estimates Were Not Clear
The secondhand-smoke estimate was weaker: pooled odds ratio 1.22, 95% confidence interval 0.69 to 2.18, and p = 0.49. Electronic nicotine products had a pooled odds ratio of 1.14, 95% confidence interval 0.82 to 1.58, and p = 0.43.
Those intervals crossed 1.0, so the review did not show a statistically clear association for those two exposure groups. That does not prove secondhand smoke or electronic nicotine products are safe for postpartum mental health; it means this evidence set was not strong enough to estimate the relationship clearly.
- Secondhand smoke: Direction was above 1.0, but the uncertainty range was wide.
- Electronic nicotine products: The pooled estimate was close to null and not statistically significant.
- Evidence gap: The paper calls for prospective studies that measure secondhand smoke and electronic nicotine products more directly.
The distinction is important for counseling. Active smoking had the clearest signal in the pooled evidence; secondhand and electronic exposure should be discussed with more caution because the review could not draw a firm conclusion from the available studies.
Pooled Postpartum Depression Prevalence Was About 15%
Across the meta-analysis, pooled postpartum depression prevalence was 0.15, with a 95% confidence interval of 0.12 to 0.17. That estimate sits close to the broad global burden often cited for postpartum depression, but the paper notes substantial variation by measurement method.
Screening tools can identify more possible cases than diagnostic interviews because they are designed to catch symptoms that may require follow-up. The review highlights that screening-based prevalence can overestimate diagnostic prevalence, so prevalence numbers need the method attached.
- Screening instruments: Better for flagging possible symptoms in larger samples, but they can include false positives.
- Diagnostic tools: More specific for clinical diagnosis, but harder to apply at scale.
- Meta-analysis pooling: Useful for a broad estimate, but sensitive to how each study measured depression.
That measurement issue does not erase the active-smoking finding. It does mean a reader should avoid treating the 15% pooled prevalence as a universal rate for every postpartum population.
High Heterogeneity Limits One-Number Interpretation
The review reported very high heterogeneity for pooled postpartum depression prevalence, with I2 = 99.80%. Heterogeneity means the included studies differed enough that one summary number cannot explain the full evidence set.
Differences in country, assessment timing, depression instrument, tobacco exposure definition, and adjustment strategy can all change the estimate. For that reason, the exposure-stratified results are more informative than the overall pooled prenatal nicotine result.
- Study design: Included studies were observational rather than randomized exposure studies.
- Timing: Postpartum depression can be measured at different points after childbirth.
- Confounding: Smoking during pregnancy may track with prior depression, stress, income, partner support, or other health risks.
- Exposure definition: Active smoking, secondhand smoke, and electronic products were not equally represented.
The safest reading is specific: prenatal active tobacco smoking was associated with higher postpartum depression odds in this evidence set. The secondhand-smoke and electronic-product questions remain open because the pooled estimates were not statistically clear.
Citation: DOI: 10.1007/s00737-026-01739-6. Sharaf-Alddin et al. Prenatal exposure to nicotine and postpartum depression: a systematic review and meta-analysis. Archives of Women’s Mental Health. 2026;29:102.
Study Design: Systematic review and random-effects meta-analysis of studies published from January 1, 2000, through September 19, 2024.
Sample Size: 29 studies in the systematic review; 26 studies in the meta-analysis.
Key Statistic: Prenatal active tobacco smoking was associated with postpartum depression with a pooled odds ratio of 1.96, 95% CI 1.59 to 2.41.
Caveat: High heterogeneity and observational designs limit causal interpretation, especially for broad pooled nicotine-exposure estimates.