TL;DR: A 2026 meta-analysis in PLOS One found clinically important sleep problems in refugee and asylum-seeking populations, with pooled sleep-adversity prevalence of 43.2% in adults and 36.4% in children and adolescents.
Key Findings
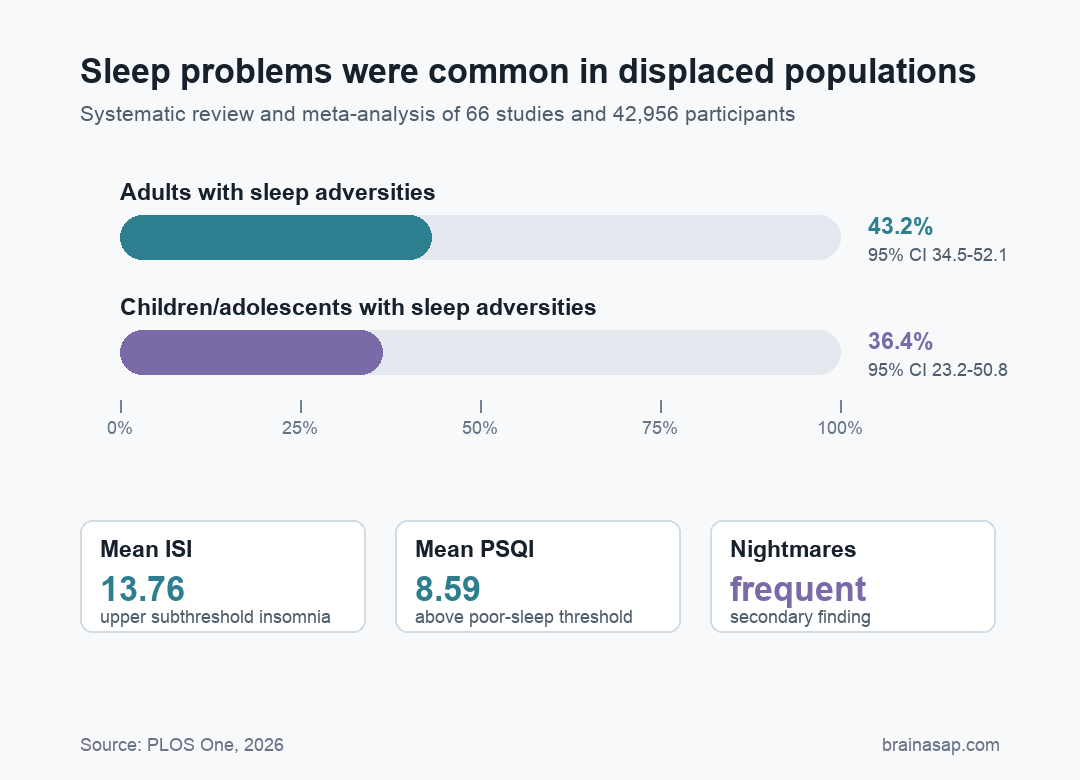
- 66 studies reviewed: The systematic review and meta-analysis covered 42,956 refugees and asylum seekers.
- 43.2% adult prevalence: Pooled sleep-adversity prevalence in adults was 43.2% (95% CI 34.5-52.1).
- 36.4% youth prevalence: Pooled sleep-adversity prevalence in children and adolescents was 36.4% (95% CI 23.2-50.8).
- ISI mean 13.76: The pooled Insomnia Severity Index score sat at the upper end of subthreshold insomnia.
- PSQI mean 8.59: The pooled Pittsburgh Sleep Quality Index score exceeded the usual threshold for poor sleep quality.
Source: PLOS One (2026) | Carpinelli et al.
Sleep disturbance is often treated as a secondary problem in displaced populations, behind housing, legal status, trauma exposure, and access to care. This review argues that sleep should be part of the core health assessment.
The paper focused on refugees and asylum seekers, groups exposed to pre-migration trauma, dangerous migration conditions, family separation, socioeconomic stress, discrimination, and uncertain settlement status.
Refugees and Asylum Seekers Had High Rates of Sleep Adversities
The authors searched Cochrane Library, Embase, and PubMed through December 2024 and included peer-reviewed studies reporting sleep quality, insomnia severity, nightmares, sleep latency, or related sleep problems.
Across 66 studies, the review included 42,956 participants. The studies covered adults, children, and adolescents from diverse origin and host regions, with conflict or war as the most common exposure context.
The review used “sleep adversities” as an umbrella term because included studies measured sleep problems in different ways. That category included insomnia symptoms, unrestorative sleep, night waking, nightmares, and other structured sleep complaints.
- Adult estimate: Sleep adversities affected 43.2% of adults, with a 95% confidence interval from 34.5% to 52.1%.
- Youth estimate: Sleep adversities affected 36.4% of children and adolescents, with a 95% confidence interval from 23.2% to 50.8%.
- Secondary problems: Prolonged sleep latency and frequent nightmares appeared across the literature.
ISI and PSQI Scores Pointed to Clinically Meaningful Sleep Problems
The pooled Insomnia Severity Index (ISI) mean was 13.76, with a 95% confidence interval of 10.39 to 17.13. That falls at the upper end of the subthreshold insomnia range and borders moderate clinical insomnia.
The pooled Pittsburgh Sleep Quality Index (PSQI) mean was 8.59, with a wide 95% confidence interval of 2.11 to 15.07. Scores above 5 are commonly used to mark poor sleep quality.
Those scores matter because sleep is not just rest time. Sleep supports emotional regulation, cognition, pain processing, cardiometabolic health, and daytime function, all of which can be strained after displacement.
Trauma, Resettlement Stress, and Healthcare Access Complicate Sleep Measurement
Refugee sleep problems rarely have one cause. The paper describes a chain of risk that can include trauma exposure before migration, unsafe conditions during displacement, and stressors after arrival in a host country.
Sleep disturbance also overlaps with PTSD, depression, anxiety, pain, and fatigue. In practice, insomnia may worsen those conditions while also being worsened by them.
- Pre-migration trauma: Violence, persecution, war, and forced displacement can increase nightmares, hyperarousal, and difficulty falling asleep.
- Post-migration stress: Housing insecurity, legal uncertainty, discrimination, unemployment, and family separation can keep sleep problems active after resettlement.
- Assessment barriers: Language, cultural adaptation, self-report cutoffs, and limited clinical access can change how sleep symptoms are reported or detected.
That complexity makes the pooled estimates useful but not precise for every setting. A refugee family in a stable resettlement program may have a different risk profile from someone in temporary housing or an asylum process with uncertain legal status.
Heterogeneity Was High Across the Sleep Literature
The main limitation was heterogeneity. Studies differed by country of origin, host country, age group, exposure type, assessment method, legal status, healthcare access, and whether PTSD-related criteria were reported.
Risk of bias also varied. Most studies had at least some concerns, and only a small share were rated low risk.
The authors also noted that many studies did not report settlement duration, education, unemployment, family separation, or follow-up data.
- Clinical tools differed: ISI, PSQI, and broader sleep-adversity measures were not interchangeable.
- Follow-up was limited: Only about 9% of studies reported follow-up data.
- Context was underreported: Time since settlement was missing in 53.0% of included studies.
- Bias concerns were common: The review rated 80.3% of studies as having some risk-of-bias concerns.
Refugee Health Protocols Should Include Sleep Screening
The practical conclusion is straightforward: refugee and asylum-seeker health assessments should ask about sleep, not only trauma, depression, and anxiety.
Different sleep presentations need different responses. Screening can identify who may need insomnia-focused care, nightmare treatment, PTSD assessment, social support, or help with safety and settlement stressors.
For health systems, sleep is a measurable entry point. Standardized sleep questions can help clinicians notice distress that may otherwise be hidden inside broad mental-health or resettlement concerns.
A sleep question can also change the next step in care. Difficulty falling asleep may point toward insomnia-focused behavioral treatment, repeated nightmares may point toward trauma-focused assessment, and sleep loss tied to housing or legal insecurity may require social support before standard therapy can work well.
That is why the paper’s recommendation is not simply to count symptoms. It is to make sleep visible in refugee health protocols so clinicians can match the response to the person’s actual sleep problem.
Citation: DOI: 10.1371/journal.pone.0352964. Carpinelli et al. Insomnia and poor sleep quality in refugee and asylum-seeking populations: A systematic review and meta-analysis. PLOS One. 2026;21(7):e0352964.
Study Design: Systematic review and meta-analysis of sleep quality and insomnia in refugee and asylum-seeking populations.
Sample Size: 66 studies with 42,956 participants.
Key Statistic: Pooled sleep-adversity prevalence was 43.2% in adults and 36.4% in children and adolescents.
Caveat: Very high heterogeneity and uneven study quality mean the pooled estimates should be interpreted as broad burden markers, not precise local rates.