TL;DR: A 2026 systematic review and meta-analysis in Journal of Sleep Research found that agomelatine modestly improved subjective sleep quality versus placebo, but objective total sleep time did not significantly increase and somnolence reports were more frequent.
Key Findings
- 25 RCTs: The review included 25 double-blind randomized controlled trials with 6,812 randomized participants.
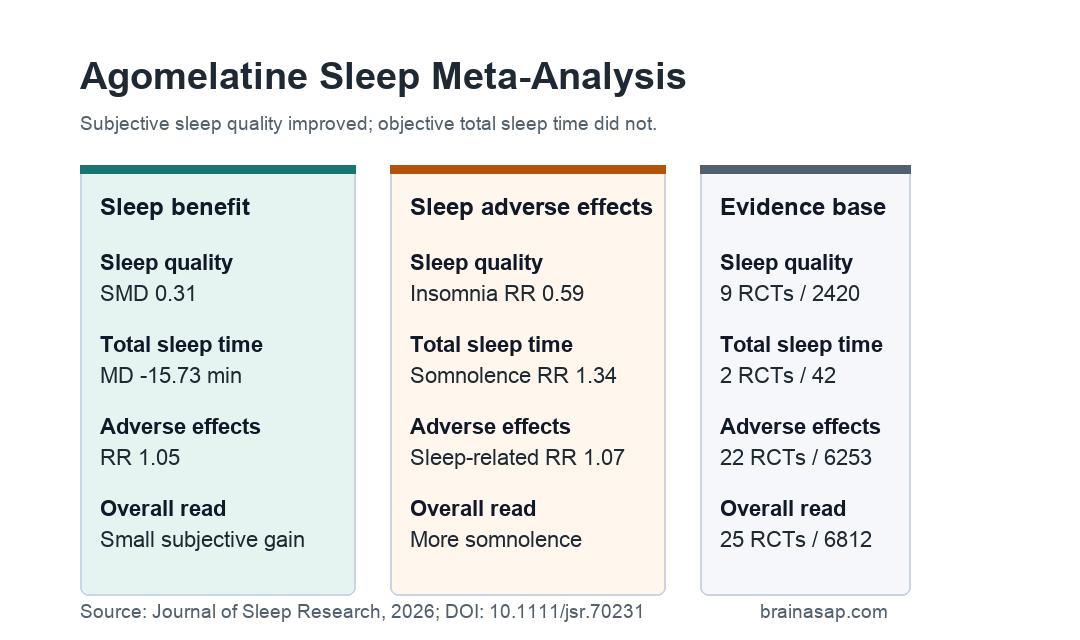
- Subjective sleep quality: Agomelatine improved patient-rated sleep quality versus placebo, SMD = 0.31, 95% CI 0.21 to 0.40.
- Objective total sleep time: 2 trials with 42 participants found no significant objective total-sleep-time effect, MD = -15.73 minutes, 95% CI -49.68 to 18.22.
- Insomnia reports: Treatment-emergent insomnia was less frequent with agomelatine, RR = 0.59, 95% CI 0.39 to 0.90.
- Somnolence reports: Treatment-emergent somnolence was more frequent with agomelatine, RR = 1.34, 95% CI 1.02 to 1.75.
Source: Journal of Sleep Research (2026) | Stefanou et al.
Agomelatine is a melatoninergic antidepressant, meaning it acts partly through melatonin-related signaling rather than functioning like a standard SSRI. Clinicians often discuss it as a medication that may help sleep disturbance, especially when sleep and mood symptoms overlap.
This meta-analysis tested that idea against placebo-controlled trial data. The strongest finding was a modest improvement in subjective sleep quality, not a clear sleep-duration gain.
Agomelatine Sleep Evidence Came From 25 Placebo-Controlled Trials
Researchers searched MEDLINE, Embase, APA PsycINFO, Cochrane Central, ClinicalTrials.gov, and WHO ICTRP up to February 16, 2025. Eligible studies were randomized controlled trials comparing agomelatine with placebo and reporting sleep-related outcomes.
The review included 25 relevant RCTs with 6,812 randomized participants. All 25 used double-blind designs, and the included studies were published between 2002 and 2024.
- Diagnoses: The trials covered major depressive disorder, generalized anxiety disorder, obsessive-compulsive disorder, bipolar disorder, autism spectrum disorder, systemic lupus erythematosus, chronic low back pain, and healthy participants.
- Design mix: 20 studies compared agomelatine and placebo as monotherapies, while 5 tested them as add-ons to another treatment.
- Participant profile: Mean age was 42.24 years, and women made up 61.23% of participants.
- Sponsorship: The review classified 72% of the included RCTs as sponsored.
The wide diagnosis mix is important for interpretation. This was not a single insomnia-disorder meta-analysis; it was a cross-population analysis of sleep outcomes reported in agomelatine trials.
Subjective Sleep Quality Improved, but the Effect Was Modest
The clearest sleep-benefit result was subjective sleep quality. Across 9 RCTs with 2,420 participants, agomelatine improved sleep-quality ratings more than placebo.
The pooled standardized mean difference was 0.31, with a 95% confidence interval from 0.21 to 0.40. In plain terms, this is a small-to-modest improvement on patient-rated sleep-quality scales, not a large sleep transformation.
- Scale type: The pooled result combined sleep-quality scales such as LSEQ and PSQI using a standardized effect size.
- Heterogeneity: Heterogeneity was low for this outcome, I2 = 5.9%.
- Prediction interval: The prediction interval was 0.13 to 0.49, suggesting future similar studies would likely remain in a small-effect range.
The review also found a small effect on subjective sleep-onset latency. Across 8 RCTs and 2,388 participants, agomelatine reduced patient-rated sleep-onset latency, SMD = -0.28, p = 0.03.
Objective Total Sleep Time Did Not Increase
The objective sleep-duration evidence was much thinner. Only 2 RCTs with 42 participants reported objective total sleep time.
That pooled result did not show a significant agomelatine benefit. The mean difference was -15.73 minutes, with a 95% confidence interval from -49.68 to 18.22 and p = 0.36.
- Total sleep time: No significant objective increase was detected.
- Objective sleep onset latency: 2 RCTs also found no significant difference, MD = 1.48 minutes, p = 0.82.
- Wake after sleep onset: 2 RCTs found no significant difference, MD = 12.22 minutes, p = 0.36.
- Awakenings: 2 RCTs found no significant difference in number of awakenings, MD = 0.70, p = 0.37.
These objective outcomes had small evidence bases. The absence of objective sleep-duration benefit should be read as limited data plus no detected effect, not proof that objective sleep outcomes are fully settled.
Insomnia Was Less Frequent, Somnolence Was More Frequent
The adverse-effect profile was mixed in a clinically predictable way. Agomelatine reduced treatment-emergent insomnia reports, but it increased treatment-emergent somnolence.
Across 7 RCTs and 2,835 participants, insomnia reports were lower with agomelatine than placebo, RR = 0.59, p = 0.01. Across 14 RCTs and 4,749 participants, somnolence reports were higher, RR = 1.34, p = 0.04.
- Lower insomnia reports: The pooled insomnia result favored agomelatine.
- Higher somnolence reports: The pooled somnolence result favored placebo.
- Global adverse effects: Across 22 RCTs and 6,253 participants, any adverse effect was slightly more frequent with agomelatine, RR = 1.05, p = 0.04.
Sleep-related adverse effects overall did not significantly differ between groups. In 17 RCTs with 5,264 participants, the pooled risk ratio was 1.07, p = 0.49.
The Result Supports Cautious Sleep-Quality Claims
This meta-analysis supports a specific claim: agomelatine can modestly improve subjective sleep quality compared with placebo across mixed trial populations. It does not support a stronger claim that agomelatine reliably increases objectively measured sleep duration.
The review also shows why sleep claims need outcome specificity. A medication can reduce insomnia complaints and improve sleep-quality ratings while also increasing somnolence and failing to lengthen objective sleep time.
Several limits should keep the result restrained. Many included trials were industry sponsored, objective sleep measures were available in only 2 small trials, and the diagnoses were mixed.
For patients, the practical question is not only whether sleep feels better. Daytime sedation, mood context, and measurable sleep change also need to fit the treatment goal.
Citation: DOI: 10.1111/jsr.70231. Stefanou et al. Effects of Agomelatine on Sleep Across Populations: A Systematic Review and Meta-Analysis. Journal of Sleep Research. 2026;35:e70231.
Study Design: Systematic review and random-effects meta-analysis of randomized placebo-controlled agomelatine trials reporting sleep outcomes.
Sample Size: 25 RCTs with 6,812 randomized participants.
Key Statistic: Subjective sleep quality improved versus placebo, SMD = 0.31, 95% CI 0.21 to 0.40; objective total sleep time did not significantly change.
Caveat: Objective sleep outcomes were reported by only 2 small RCTs, and the included trial populations were clinically mixed.