TL;DR: A 2026 case study in Neurological Sciences described 2 Tourette syndrome patients who developed oculogyric crisis, a sustained upward eye-rolling dystonia, after aripiprazole was increased to 20-30 mg/day, with both cases resolving after dose reduction.
Key Findings
- 2 Tourette cases: The report described 2 female patients, ages 16 and 22, treated with aripiprazole for chronic motor and vocal tics.
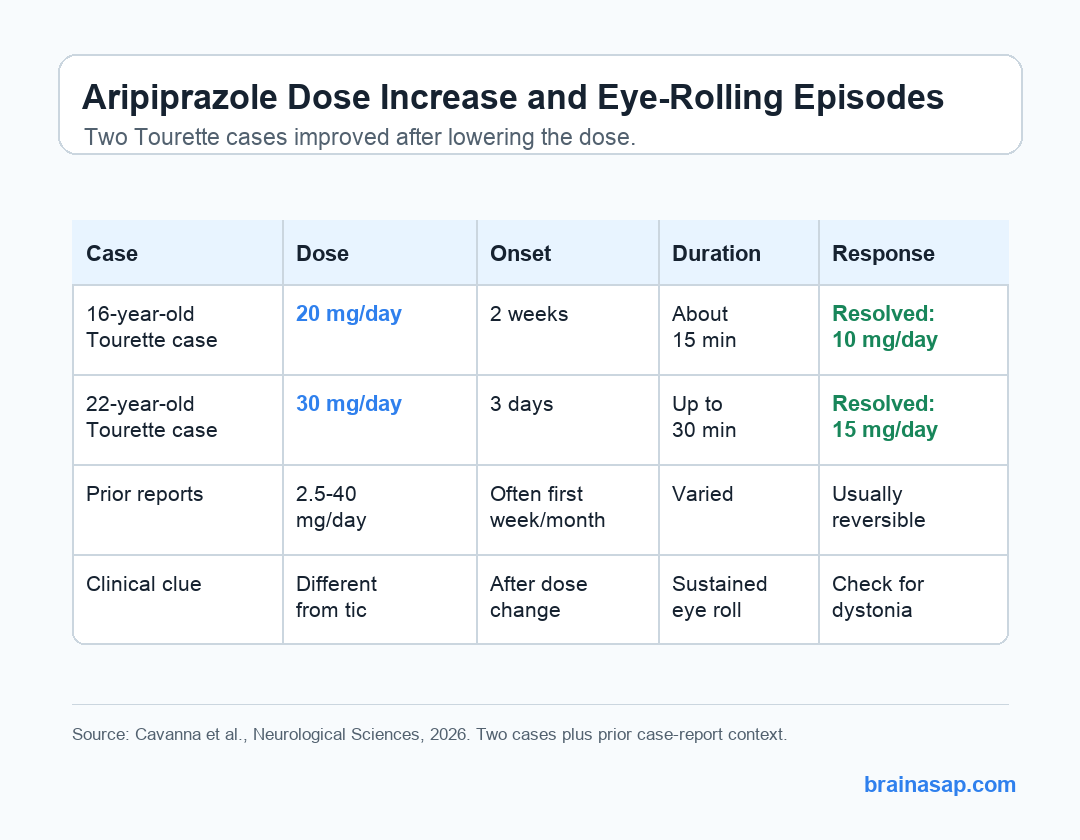
- 20-30 mg/day exposure: Oculogyric crisis appeared after aripiprazole reached 20 mg/day in one patient and 30 mg/day in the other.
- 15-30 minute episodes: The eye-rolling spells lasted about 15 minutes in the younger patient and up to 30 minutes in the older patient.
- Dose reduction resolved symptoms: Reducing aripiprazole to 10 mg/day or 15 mg/day was followed by remission of the oculogyric crisis in both cases.
- 18 prior cases reviewed: Researchers identified 18 earlier aripiprazole-related oculogyric crisis cases, with most resolving after discontinuation, dose reduction, or anticholinergic treatment.
Source: Neurological Sciences (2026) | Cavanna et al.
Aripiprazole is often used in Tourette syndrome because it can reduce tics while avoiding some metabolic, prolactin, and cardiac side effects associated with older antidopaminergic drugs.
This case report adds a narrower safety point: even a medication with a generally favorable tolerability profile can produce a rare acute dystonic reaction when the dose is raised.
Oculogyric Crisis Looked Different From the Patients’ Tics
Oculogyric crisis is a dystonic reaction in which extraocular muscles contract in a sustained, spasmodic way, often producing upward eye deviation. In these 2 patients, the episodes were clinically different from their usual motor tics.
The distinction was important because Tourette syndrome already involves repeated movements. The report emphasized several features that separated the new episodes from the patients’ established tic pattern:
- No premonitory urge: The eye-rolling episodes were not preceded by the inner urge that often comes before a tic.
- Sustained eye deviation: The episodes involved upward eye rolling lasting minutes rather than brief tic-like movements.
- Temporal link to dose escalation: Each case emerged shortly after reaching a higher aripiprazole dose.
- Improvement after dose reduction: Symptoms remitted after aripiprazole was lowered, without a full medication switch in either case.
The younger patient had marked tic severity, with a 100% Tourette Syndrome Diagnostic Confidence Index score and an 80% Yale Global Tic Severity Scale score. After gradual titration to 20 mg/day, she developed upward eye-rolling episodes that lasted about 15 minutes.
Lowering aripiprazole to 10 mg/day was followed by resolution. No additional medication switch was needed.
A Second Patient Developed Weekly Eye-Rolling Episodes at 30 mg/day
The older patient had moderate tic severity, with a 73% diagnostic confidence score and a 51% Yale Global Tic Severity Scale score. She had not previously received pharmacotherapy for her tics.
Her aripiprazole was titrated from 5 mg/day to 30 mg/day in 5 mg steps. 3 days after reaching 30 mg/day, she developed weekly upward eye-rolling episodes lasting up to 30 minutes.
Procyclidine, an anticholinergic medication used for some dystonic reactions, did not stop the episodes even at up to 20 mg/day. Symptom remission followed aripiprazole dose reduction to 15 mg/day.
The Earlier Case Literature Also Points to Early-Onset, Reversible Events
Researchers reviewed 18 previously reported cases of aripiprazole-related oculogyric crisis. The earlier cases involved patients ages 11 to 28 years, and half were female.
Only 2 of the 18 earlier cases involved people taking aripiprazole for a tic disorder. Other indications included psychosis, affective disorders, obsessive-compulsive disorder, autism spectrum disorder, attention-deficit/hyperactivity disorder, and borderline personality disorder.
The timing pattern was clinically relevant:
- First week: Eight earlier cases developed oculogyric crisis within the first week of treatment.
- First month: Six additional cases developed it within the first month.
- 2.5-40 mg/day range: Reported aripiprazole doses varied widely, so dose alone did not fully explain risk.
- Mostly reversible: All but one earlier case resolved after medication discontinuation, dose reduction, or anticholinergic treatment.
In the 2 new Tourette cases, the timing was especially tied to reaching the target dose. One patient developed symptoms 2 weeks after reaching 20 mg/day; the other developed symptoms 3 days after reaching 30 mg/day.
Dopamine Modulation May Help Explain the Reaction
Aripiprazole has a mixed receptor profile. It acts partly at dopamine D2/D3 receptors and serotonin 5-HT1A receptors, while also blocking serotonin 5-HT2A receptors.
The brief communication did not prove a mechanism, but it offered a plausible clinical interpretation. Aripiprazole modulates dopaminergic activity and lacks anticholinergic effects, a combination that may leave some patients vulnerable to extrapyramidal side effects such as dystonia.
Clinical monitoring should focus on a specific pattern:
- Small evidence base: A case report cannot estimate how often this adverse effect occurs.
- Watch the dose-change window: New sustained eye deviation after titration deserves attention, especially when it differs from usual tics.
- Separate tics from dystonia: Premonitory urges, suppressibility, duration, and muscle pattern can help distinguish a tic from oculogyric crisis.
- Dose reduction may be enough: In both reported Tourette cases, symptoms resolved after lowering aripiprazole rather than stopping it entirely.
The monitoring point is narrow: new sustained eye deviation after dose escalation should be evaluated as possible dystonia, while ordinary tic fluctuations still need clinical context.
The Main Limit Is the Small Case-Report Design
The evidence base here is intentionally narrow. The paper reported 2 new cases and placed them beside published case literature, not a prospective Tourette syndrome cohort.
That design is useful for detecting a rare, clinically recognizable adverse event, but it cannot separate dose effects from individual susceptibility, co-medications, or the clinical reasons dose escalation was needed.
The safest reading is therefore straightforward: in Tourette syndrome patients taking aripiprazole, new sustained upward eye-rolling episodes after dose escalation should prompt evaluation for oculogyric crisis, particularly when the episodes lack the usual tic urge and last much longer than typical tics.
Citation: DOI: 10.1007/s10072-026-09056-7. Cavanna et al. Oculogyric crisis in 2 patients treated with aripiprazole for chronic tics. Neurological Sciences. 2026;47:450.
Study Design: Brief communication with 2 Tourette syndrome case reports plus review of prior aripiprazole-related oculogyric crisis cases.
Sample Size: 2 new patients, ages 16 and 22, with 18 previously reported cases summarized for context.
Key Statistic: Both new cases resolved after aripiprazole dose reduction; earlier cases were reversible in all but one published report.
Caveat: Case reports can identify a plausible adverse drug reaction but cannot estimate incidence or prove dose-dependent risk.





