TL;DR: A 2026 study in O&G Open found that cannabis exposure 2–7 years after a first pregnancy was not associated with incident hypertension after adjustment in the nuMoM2b Heart Health Study.
Key Findings
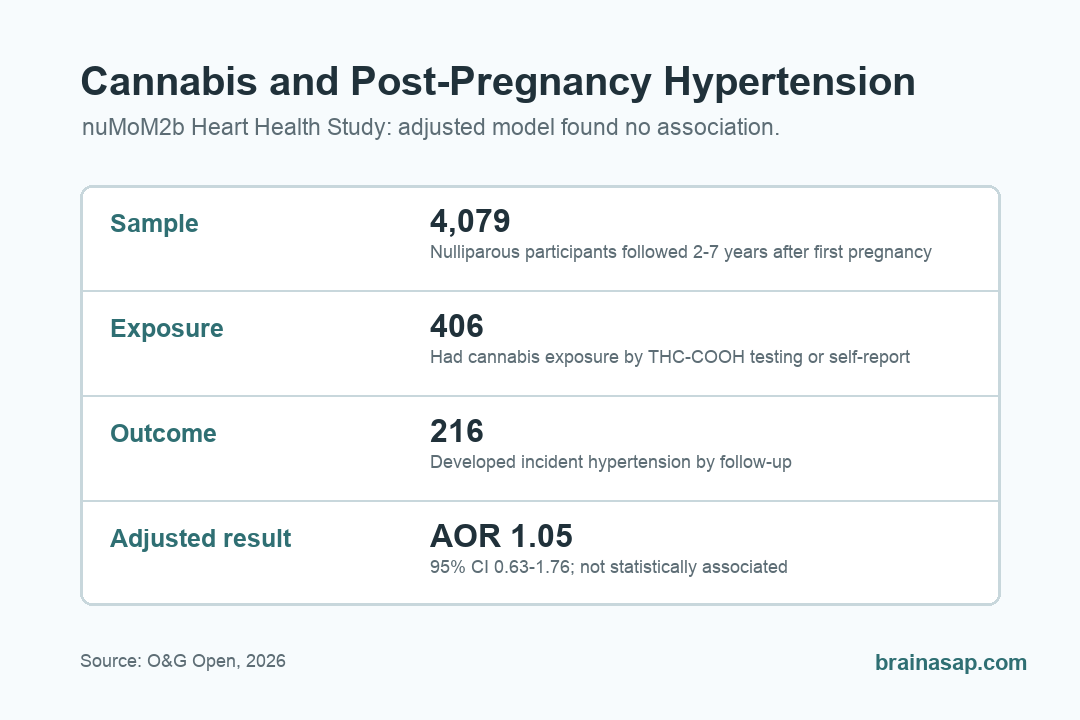
- No adjusted hypertension association: Cannabis exposure was not associated with incident hypertension after adjustment (AOR 1.05; 95% CI, 0.63-1.76).
- 4,079-person analysis: Researchers analyzed nulliparous participants from the nuMoM2b Heart Health Study 2–7 years after a first pregnancy.
- 10.0% had cannabis exposure: Cannabis exposure was detected in 406 participants by urine THC-COOH testing or self-report at follow-up.
- Cardiovascular risk has direct brain-health implications: Hypertension in midlife is one of the strongest modifiable risk factors for late-life dementia, stroke, and cognitive decline — making post-pregnancy cardiovascular risk a brain-health concern.
- Cross-sectional secondary analysis: The design captures associations rather than causal relationships; cannabis use and hypertension may share upstream factors (stress, lifestyle, socioeconomic context) that the analysis tries to account for.
Source: O&G Open (2026) | Dahl et al.
The cannabis research landscape has been dominated by two endpoints: acute use effects (intoxication, cognition, accident risk) and prenatal exposure effects (developmental outcomes for the child). Less work has examined what cannabis use in adult women predicts for their own cardiovascular and brain health years downstream.
The nuMoM2b Heart Health Study tracked nulliparous (first-pregnancy) women for years after their initial pregnancy and provides a relatively clean window onto post-pregnancy cardiovascular outcomes.
Why Post-Pregnancy Cardiovascular Health Is a Brain-Health Question
The connection between cardiovascular risk and brain health is well-established but often missed in clinical conversations:
- Midlife hypertension is one of the strongest modifiable predictors of late-life dementia. Decades of cohort studies show that elevated blood pressure in midlife substantially raises Alzheimer’s and vascular dementia risk in later life.
- Hypertension contributes to white matter disease, microinfarcts, and small-vessel pathology that accumulate over decades and shape cognitive trajectories.
- Stroke risk — major contributor to cognitive impairment and dementia — is driven heavily by hypertension.
- Hypertensive disorders of pregnancy (preeclampsia, gestational hypertension) flag long-term cardiovascular and brain-health risk that often goes unaddressed in postpartum follow-up.
The nuMoM2b Heart Health Study was designed to follow women’s cardiovascular trajectories through the post-pregnancy period when these risks consolidate. Examining what predicts incident hypertension in that window has direct implications for downstream cognitive outcomes — not just cardiovascular ones.
How the nuMoM2b Heart Health Study Was Designed for This Question
The nuMoM2b cohort tracked first-pregnancy women through pregnancy and into the years afterward, with a parallel Heart Health Study assessment during the post-pregnancy period:
- Nulliparous baseline: Participants were nulliparous (no previous pregnancy) at study entry, providing a clean cardiovascular baseline before pregnancy-related changes.
- 2-7 year follow-up window: Heart Health Study assessment captured the period when post-pregnancy lifestyle patterns and cardiovascular risks consolidate.
- Cannabis exposure assessment: Use patterns post-pregnancy were measured and related to subsequent cardiovascular outcomes.
- Hypertension as primary outcome: Incident hypertension — a clinically meaningful and well-measured cardiovascular endpoint — was the focus.
Why Postpartum Cardiovascular Risk Often Falls Through the Cracks
Postpartum care in the US is typically condensed into a single 6-week visit followed by routine well-woman care. This gap leaves a critical cardiovascular monitoring window underserved:
- Hypertensive disorders of pregnancy double or triple lifetime cardiovascular risk but postpartum follow-up is often inadequate to track that elevated risk.
- New-onset hypertension in the years after pregnancy often emerges before patients have established a pattern of routine cardiovascular checks.
- Lifestyle changes after pregnancy — sleep disruption, weight retention, stress patterns, substance use — can produce cardiovascular risk in patterns clinicians don’t routinely ask about.
- Cannabis use specifically has risen substantially with legalization, including among women in reproductive years and beyond, but cardiovascular implications are often not part of routine clinical conversations.
The Dahl analysis adds evidence to a broader case for more systematic post-pregnancy cardiovascular monitoring, while also showing why cannabis counseling should not overstate this specific hypertension result.
Why Cannabis-Hypertension Connections Are Plausible Biologically
Several mechanisms could connect cannabis use to elevated blood pressure over time:
- Acute cannabis-cardiovascular effects: Cannabis acutely raises heart rate and can affect blood pressure regulation in complex ways depending on dose and chronicity.
- Inflammation and vascular function: Chronic cannabis use has been associated in some studies with inflammatory markers and endothelial function changes.
- Lifestyle clustering: Cannabis use can travel with other lifestyle factors (sleep disruption, dietary patterns, stress regulation differences) that independently affect cardiovascular risk.
- Sympathetic nervous system effects: Cannabis affects autonomic regulation in ways that could plausibly shape long-term blood pressure trajectories.
The mechanistic literature is genuinely mixed — cannabis is not a textbook hypertension risk factor like sodium, alcohol, or sedentary lifestyle. This null finding is part of why clean cohort studies of cannabis-cardiovascular outcomes matter.
The Dahl analysis contributes one adjusted null result to a sparse literature on this specific exposure window.
The Honest Limits of Cross-Sectional Cohort Analysis
- Cross-sectional design captures associations, not causal relationships. Whether cannabis use causes hypertension or whether both reflect upstream factors (stress, lifestyle, socioeconomic context, mental health) the analysis cannot fully disentangle.
- Self-reported cannabis use has measurement error. Underreporting in observational studies is well-documented and probably affects effect-size estimation.
- Cannabis use patterns vary substantially. Frequency, dose, route of administration, THC content, and concurrent tobacco use all affect cardiovascular impact in ways aggregate “ever-use” measures can’t capture.
- Confounding by lifestyle factors is hard to fully address. People who use cannabis differ from non-users in many ways that could independently affect cardiovascular risk.
- Generalization beyond first-pregnancy women requires separate testing — the nuMoM2b sample is by design nulliparous-at-baseline.
What This Should Add to Postpartum Counseling Conversations
Clinical implication: postpartum cardiovascular counseling can include cannabis exposure while stating clearly that this study did not find an independent hypertension association.
- Cannabis use should be part of postpartum cardiovascular risk discussions. Routine clinical conversations about smoking, alcohol, exercise, and diet should include cannabis — especially for women who used or began using cannabis after their first pregnancy.
- Post-pregnancy hypertension monitoring matters for brain health, not just cardiovascular outcomes. Midlife blood pressure shapes late-life dementia risk, and early identification of elevated blood pressure allows lifestyle and medication intervention before damage accumulates.
- Cannabis is no longer a niche substance. Legalization has normalized use among women in their 30s and 40s, and clinical conversations need to keep pace with that shift.
- Risk counseling should be specific. “Cannabis raises hypertension risk” is too blunt — the nuanced picture (frequency, dose, individual cardiovascular baseline, concurrent risk factors) is what actually informs decisions.
Brain-health interpretation: The dementia-prevention research community has converged on a clear message: midlife cardiovascular risk factors are among the most modifiable contributors to late-life cognitive outcomes. The Lancet Commission on dementia prevention identifies hypertension, smoking, obesity, and several other midlife factors as key targets for cognitive risk reduction.
Cannabis has not featured prominently in these prevention frameworks because the cardiovascular evidence has been mixed and small-scale. The Dahl analysis adds a large post-pregnancy null result to that evidence base.
Practical interpretation: this analysis did not support cannabis exposure 2–7 years after first pregnancy as an independent hypertension predictor. It supports measuring postpartum cardiovascular risk directly instead of assuming cannabis exposure explains later hypertension.
Citation: DOI: 10.1097/og9.0000000000000164. Dahl et al. Cannabis Exposure After Pregnancy and Development of Hypertension in the nuMoM2b Heart Health Study. O&G Open. 2026.
Study Design: Secondary cross-sectional analysis of the nuMoM2b Heart Health Study examining cannabis exposure 2–7 years after a first pregnancy and association with incident hypertension; nulliparous baseline cohort.
Sample Size: 4,079 participants; 406 had cannabis exposure and 216 developed hypertension by the 2–7 year follow-up visit.
Key Statistic: Cannabis exposure was not associated with incident hypertension after adjustment (AOR 1.05; 95% CI, 0.63-1.76).
Caveat: Cross-sectional secondary analysis cannot establish causality; self-reported cannabis use carries measurement error; lifestyle confounding is incompletely addressable; nulliparous-at-baseline cohort design limits generalization beyond first-pregnancy women.