TL;DR: A 2026 study in Critical Care Explorations described a 45-year-old woman whose extended-release carbamazepine and venlafaxine overdose led to cardiac arrest, delayed serotonin syndrome, rebounding carbamazepine levels, bowel ischemia, and right hemicolectomy after retained gastrointestinal drug material kept releasing medication.
Key Findings
- Extended-release overdose: The patient had altered mental status after a carbamazepine-venlafaxine ER overdose and an initial carbamazepine concentration of 163 micromol/L.
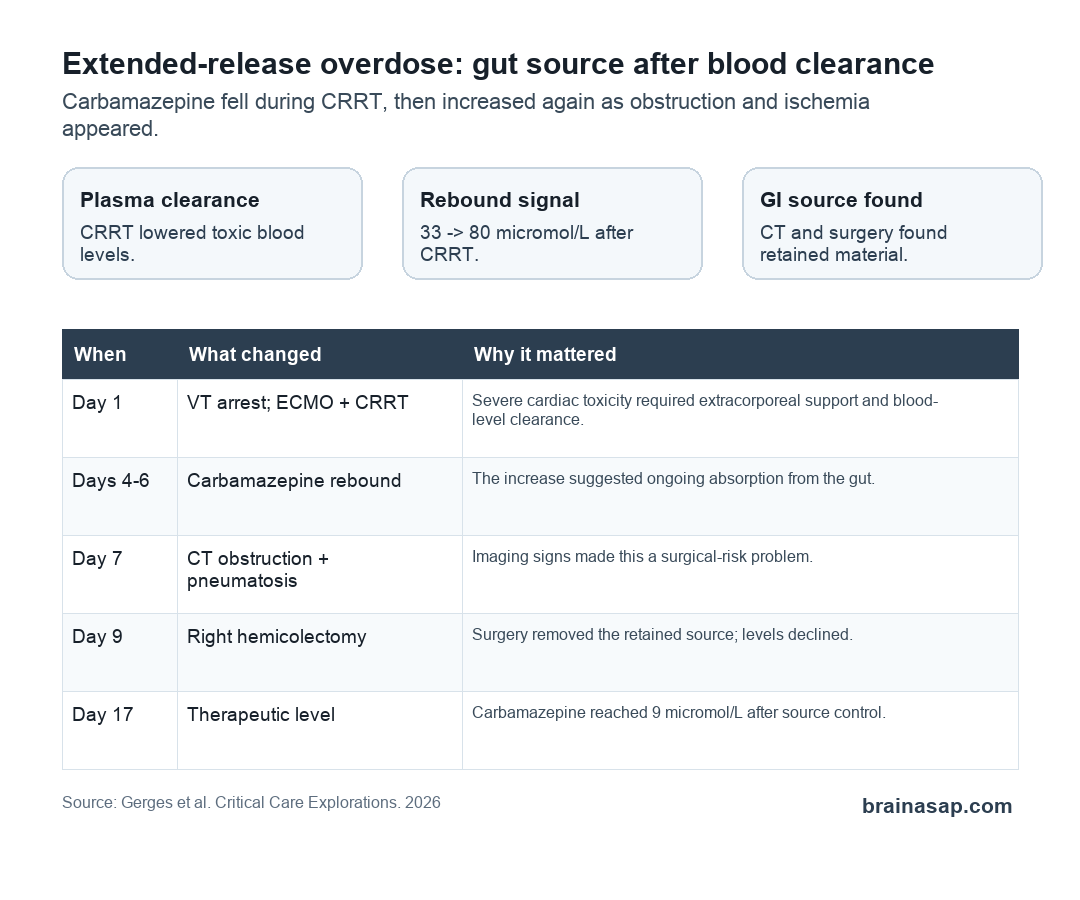
- Cardiac toxicity: She developed ventricular tachycardia arrest, required 13 minutes of resuscitation, and was placed on venoarterial ECMO plus CRRT.
- Drug-level rebound: After CRRT, carbamazepine rebounded from 33 to 80 micromol/L, suggesting continued gastrointestinal absorption.
- Bowel warning signs: CT showed terminal-ileum high-density material, bowel dilation, a transition point, and cecal pneumatosis consistent with ischemia.
- Surgical source control: Day 9 laparotomy found transmural ischemic necrosis and 4-6 L of retained charcoal/polyethylene glycol mixture, requiring right hemicolectomy.
Source: Gerges et al. Critical Care Explorations. 2026.
Extended-release overdose can be dangerous for a reason that ordinary blood-clearing treatments do not fully solve: medication can remain inside the gastrointestinal tract and keep dissolving.
In this case report, that problem appeared after a severe overdose involving carbamazepine ER, an antiseizure medication, and venlafaxine ER, an antidepressant. Both can cause serious toxicity in overdose, and both extended-release formulations can create prolonged absorption.
Carbamazepine Toxicity Rebounded After Blood Clearance
The patient was a 45-year-old woman with refractory epilepsy and depression. She arrived after intentional overdose with altered mental status and empty medication bottles nearby; about 40 venlafaxine tablets were missing.
Her Glasgow Coma Scale score fell from 13 to 6, prompting intubation and mechanical ventilation. A carbamazepine concentration drawn about 3 hours after arrival was 163 micromol/L, far above the paper’s toxic threshold of more than 64 micromol/L.
The early cardiac findings also showed severe toxicity:
- QRS widening: The electrocardiogram showed a QRS duration of 166 ms.
- QTc prolongation: QTc reached 530 ms, increasing concern for dangerous rhythm problems.
- Initial decontamination: Clinicians gave 50 g of activated charcoal, but multidose charcoal was limited by hemodynamic instability.
8 hours after arrival, she had ventricular tachycardia arrest. Resuscitation included shocks, sodium bicarbonate, calcium chloride, magnesium sulfate, and epinephrine before clinicians escalated to venoarterial extracorporeal membrane oxygenation (ECMO) and continuous renal replacement therapy (CRRT).
CRRT helped clear carbamazepine from blood. After 24 hours, the level had fallen to 92 micromol/L, and later it dropped as low as 33 micromol/L.
That improvement did not hold. 4 days after ECMO decannulation and CRRT discontinuation, the patient developed hyperreflexia, fever, and clonus, signs consistent with serotonin syndrome, even though she was no longer receiving carbamazepine or venlafaxine.
Whole Bowel Irrigation Produced Little Output
Clinicians attempted whole bowel irrigation with 8 L of polyethylene glycol. The response was not what they expected: nasogastric output was only about 500 mL, mostly retained charcoal.
That limited output mattered because whole bowel irrigation depends on moving material through the gut. When the bowel is not moving normally, retained medication, activated charcoal, and lavage fluid can remain trapped rather than being eliminated.
The case then showed three linked warning signs:
- Drug rebound: Carbamazepine increased from 33 to 80 micromol/L after CRRT stopped.
- Persistent neurologic toxicity: Clonus and other serotonin-syndrome features persisted.
- Abdominal deterioration: Progressive distension, absent bowel sounds, and peritonitis developed.
The researchers interpreted the rebound as evidence that drug was still entering the bloodstream from the gut. CRRT could remove carbamazepine from plasma, but it could not remove a continuing intestinal source.
CT Pointed to Retained Drug Material and Ischemia
Abdominal CT showed high-density material in the terminal ileum, bowel dilation up to 3.9 cm, and cecal pneumatosis. Pneumatosis means gas in the bowel wall, a finding that can signal ischemia when it appears with the right clinical picture.
The scan also suggested a transition point near the ileocecal valve, consistent with partial bowel obstruction. In practical terms, the imaging connected the blood-level rebound to a likely intestinal reservoir.
The paper describes a “functional pharmacobezoar.” A pharmacobezoar is a mass or retained collection of medication inside the gastrointestinal tract. In this case, clinicians did not find intact pill fragments during surgery, but the retained material and rebound kinetics supported ongoing drug sequestration and release.
Several mechanisms could have overlapped:
- Extended-release matrix: ER tablets can keep releasing medication after ingestion.
- Reduced gut movement: Carbamazepine’s anticholinergic effects can impair motility.
- Critical illness: Cardiac arrest, shock physiology, and ECMO flow changes may worsen bowel perfusion.
- Distension: Retained charcoal and polyethylene glycol can add volume when bowel transit fails.
Surgery Stopped the Ongoing Source
On hospital day 9, exploratory laparotomy found transmural ischemic necrosis of the cecum and ascending colon. When the necrotic bowel was mobilized, it perforated and released 4-6 L of charcoal/polyethylene glycol mixture combined with feces.
Surgeons performed a right hemicolectomy and peritoneal irrigation. A temporary abdominal closure was followed 48 hours later by fascial closure, end ileostomy, and mucous fistula.
Pathology confirmed severe acute transmural ischemic colitis with fibrin thrombi in mesenteric vessels.
After surgery, carbamazepine levels declined more steadily. The concentration fell to 56 micromol/L postoperatively and reached a therapeutic level of 9 micromol/L by day 7 after surgery, or day 17 after overdose.
Clonus resolved as the drug level fell, and neurocognition gradually recovered. The patient was discharged to rehabilitation and then home after 3 months.
Drug-Level Rebound Should Trigger a GI Source Search
The clinical lesson is not that every extended-release overdose requires surgery. The point is narrower: when drug levels rebound after apparently adequate blood clearance, clinicians should look for ongoing gastrointestinal absorption.
The report highlights several findings that should raise concern:
- Rebounding concentration: A rising drug level after CRRT suggests continued absorption rather than only slow redistribution.
- Failed bowel output: Whole bowel irrigation with minimal output can indicate retained material or poor transit.
- Abdominal signs: Distension, absent bowel sounds, peritonitis, or worsening pain change the problem from toxicology alone to possible surgical disease.
- Imaging signs: High-density intraluminal material, obstruction, pneumatosis, or ischemia should prompt urgent surgical evaluation.
The case also shows why extracorporeal treatment has a boundary. CRRT can lower plasma carbamazepine, but it cannot stop an extended-release intestinal reservoir from feeding more drug into the bloodstream.
The main takeaway is direct: in severe extended-release overdoses, the gut can remain an active drug source long after blood levels first improve. A rebound level plus abdominal deterioration is a different warning pattern from ordinary slow recovery.
Citation: DOI: 10.1097/cce.0000000000001395. Gerges Gerges et al. Functional Pharmacobezoar and Bowel Ischemia Requiring Hemicolectomy Complicating Extended-Release Carbamazepine-Venlafaxine Overdose. Critical Care Explorations . 2026;8:e1395. Critical Care Explorations. 2026.
Study Design: Critical-care case report of an extended-release carbamazepine-venlafaxine overdose.
Sample Size: 1 45-year-old woman treated after intentional overdose.
Key Statistic: Carbamazepine rebounded from 33 to 80 micromol/L after CRRT stopped, then declined after surgical evacuation and right hemicolectomy.
Caveat: A single case report can identify a warning pattern but cannot estimate how often this complication occurs.