TL;DR: A 2026 medRxiv preprint found that a composite cerebral small vessel disease (cCSVD) score from routine T1 MRI predicted 3-month cognitive recovery after stroke better than any single small-vessel marker in a 65-person cohort.
Key Findings
- Recovery window: The study analyzed 65 early subacute stroke survivors who completed baseline and 90-day follow-up visits.
- MRI score: The cCSVD score combined white matter hyperintensity volume, perivascular space count, and brain-predicted age difference from baseline T1 MRI.
- Shared MRI pattern: The first principal component explained 43.1% of variance across the 3 imaging markers.
- Follow-up cognition: Lower baseline cCSVD was linked to better follow-up Montreal Cognitive Assessment (MoCA) scores after accounting for baseline MoCA.
- Recovery threshold: Among people cognitively impaired at baseline, lower cCSVD also predicted greater odds of improving to cognitively unimpaired status by 3 months.
Source: medRxiv preprint, 2026.
Stroke recovery is often judged from the visible injury: the infarct location, infarct volume, and early functional deficits. Researchers tested a wider idea: cognitive recovery may also depend on the condition of the rest of the brain.
Researchers focused on cerebral small vessel disease (CSVD), a group of MRI-visible changes tied to several brain-health domains:
- Aging: whether brain structure looks older than expected.
- Vascular injury: whether white matter shows chronic small-vessel damage.
- Tissue integrity: whether the brain has enough structural reserve for recovery.
Instead of treating one marker as the whole story, they built a composite score that pulled 3 related measurements into one brain-health index.
Cognitive Recovery After Stroke Was Measured With MoCA
The cohort included 65 stroke survivors recruited from Casa Colina Hospital, Emory University, and NYU Langone Health. Participants had early subacute stroke with upper-extremity motor impairment and completed both baseline and follow-up visits.
Baseline visits occurred about 24.0 days after stroke on average. Follow-up visits occurred about 96.1 days after stroke, leaving roughly a 3-month recovery window.
Cognition was measured with the Montreal Cognitive Assessment (MoCA), a brief screening test used to capture global cognitive performance. Scores ranged from 0 to 28 at baseline and from 0 to 29 at follow-up, with 2 participants excluded from MoCA analyses because they did not complete both assessments.
The imaging side used baseline T1-weighted MRI. Researchers automatically quantified 3 markers before combining them:
- White matter hyperintensity volume: an MRI marker of vascular injury in white matter.
- Perivascular space count: a marker the researchers used as a proxy for small-vessel and fluid-clearance burden.
- Brain-predicted age difference: a structural atrophy marker that estimates whether a brain appears older or younger than expected for chronological age.
Each imaging marker was residualized for age, sex, days since stroke, and intracranial volume before the composite was built. This kept the score focused on disease-related structural integrity, not just age or head-size differences.
The Composite Small Vessel Disease Score Balanced Three MRI Markers
The researchers used principal component analysis (PCA) to derive the composite cerebral small vessel disease score. PCA is a statistical method that finds shared patterns across related measurements.
Here, PCA asked whether 3 different MRI markers carried a common small-vessel-disease signal:
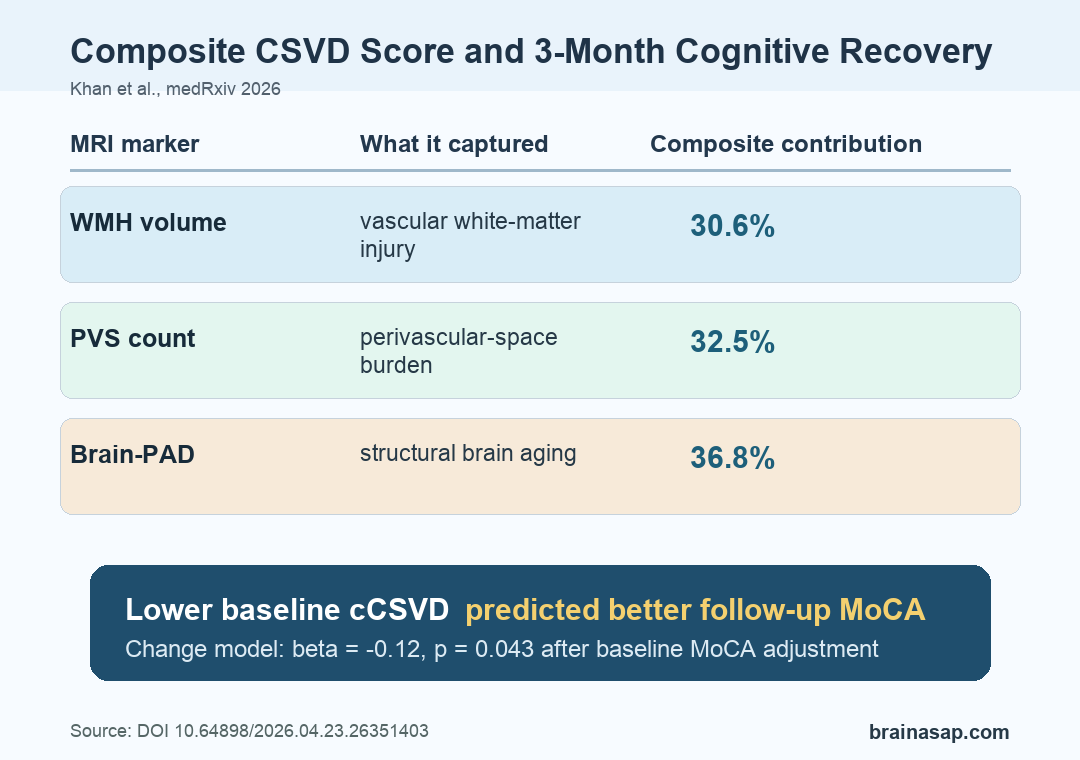
- WMH volume: vascular white-matter injury.
- PVS count: perivascular-space burden.
- Brain-PAD: structural brain aging.
The first principal component explained 43.1% of total variance. The 3 markers contributed in a relatively balanced way: white matter hyperintensity volume contributed 30.6%, perivascular space count contributed 32.5%, and brain-predicted age difference contributed 36.8%.
That balance is the central technical result. The composite was not just a disguised version of one measure.
It captured a shared MRI pattern across vascular injury, perivascular-space burden, and structural brain aging.
The study then asked whether this cCSVD score predicted cognitive status at baseline, cognitive status at follow-up, and follow-up cognition after accounting for baseline MoCA. Stability selection with LASSO helped select predictors for the regression models.
Lower cCSVD Predicted Better Follow-Up MoCA Scores
Lower baseline cCSVD was associated with better follow-up MoCA performance. In the follow-up model, the cCSVD coefficient was beta = -0.19 with p = 0.009.
In the change model, which adjusted for baseline MoCA, the cCSVD coefficient remained significant at beta = -0.12 with p = 0.043.
Those negative coefficients mean that a higher small-vessel-disease burden was linked to worse cognitive recovery, while a lower burden was linked to better recovery. The result stayed visible even when the model accounted for a person’s starting cognitive score.
The analysis also compared the composite with individual biomarkers. In this cohort, cCSVD outperformed the single markers as a predictor of longitudinal cognitive change.
The recovery pattern had 3 parts:
- Whole-brain condition mattered: Follow-up cognition was not explained only by the focal stroke lesion.
- Composite MRI burden mattered: The combined score appeared more robust than white matter hyperintensity, perivascular spaces, or brain age alone.
- Baseline cognition still mattered: Baseline MoCA was a strong predictor in the change model, but it did not remove the cCSVD association.
In a separate logistic model among participants who were cognitively impaired at baseline, lower cCSVD predicted a greater chance of improving to cognitively unimpaired status by 3 months. The reported odds ratio was 0.34 with p = 0.036, independent of age and education.
Why a Composite MRI Score May Help After Stroke
Post-stroke cognitive recovery depends on more than the damaged tissue visible at the lesion site. A person also needs enough remaining network integrity to support compensation, learning, attention, and daily cognitive function during recovery.
The cCSVD framework fits that biology because each marker reflects a different part of brain structural health:
- Vascular injury: White matter hyperintensities can reflect chronic small-vessel damage that disrupts communication pathways.
- Clearance and small-vessel burden: Perivascular-space counts may reflect altered fluid clearance or small-vessel pathology.
- Structural atrophy: Brain-predicted age difference captures whether the brain’s structure appears older than expected.
Combining those markers may identify patients whose brains have less reserve for cognitive recovery after stroke. The study authors argue that a composite T1-based score could be scalable because the required scan type is common and the measurements can be automated.
That does not make cCSVD a clinical decision tool yet. The research is a preprint, the sample was modest, and the cohort was selected around motor impairment.
The score also used 3 imaging markers rather than the full range of small-vessel-disease features. Future versions could add lacunes, microbleeds, or cortical superficial siderosis if automated detection tools are reliable enough.
The narrower conclusion is still useful: in this dataset, a balanced MRI composite of small-vessel disease was linked to who recovered cognitively over the next 3 months.
Small-Vessel Disease May Limit Cognitive Recovery After Stroke
The study points toward a more whole-brain view of recovery prediction. Focal lesion features remain important, but they may not fully explain why two people with similar strokes recover differently.
A useful next test would be a larger externally validated cohort with broader small-vessel-disease features, more detailed cognitive outcomes, and longer follow-up. That would show whether cCSVD remains predictive across scanner types, stroke subtypes, rehabilitation settings, and patient populations.
For now, the result supports a measured claim: baseline small-vessel-disease burden, summarized across several MRI markers, may help explain short-term cognitive recovery after stroke.
Citation: DOI: 10.64898/2026.04.23.26351403. Khan et al. A composite measure of cerebral small vessel disease predicts cognitive change after stroke. medRxiv. 2026.
Study Design: Prospective observational analysis of stroke survivors with baseline MRI and 90-day cognitive follow-up.
Sample Size: 65 early subacute stroke survivors completed both visits; 62 were included in MoCA regression analyses.
Key Statistic: Lower baseline cCSVD predicted better follow-up MoCA after baseline adjustment (beta = -0.12, p = 0.043).
Caveat: This is a non-peer-reviewed preprint from a modest cohort, so the composite needs external validation before clinical use.





