TL;DR: A 2026 preprint in medRxiv found that the ADAS-Cog-13 cognitive scale detected impairment in older adults with focal epilepsy, but a cutoff of 15 had only modest diagnostic accuracy against an epilepsy-specific neuropsychological standard.
Key Findings
- 83 epilepsy patients: The study analyzed adults older than 55 with focal epilepsy from the Brain, Aging, and Cognition in Epilepsy cohort.
- 83 matched controls: Each epilepsy participant was matched to a cognitively healthy Alzheimer Disease Neuroimaging Initiative control by age, sex, and education.
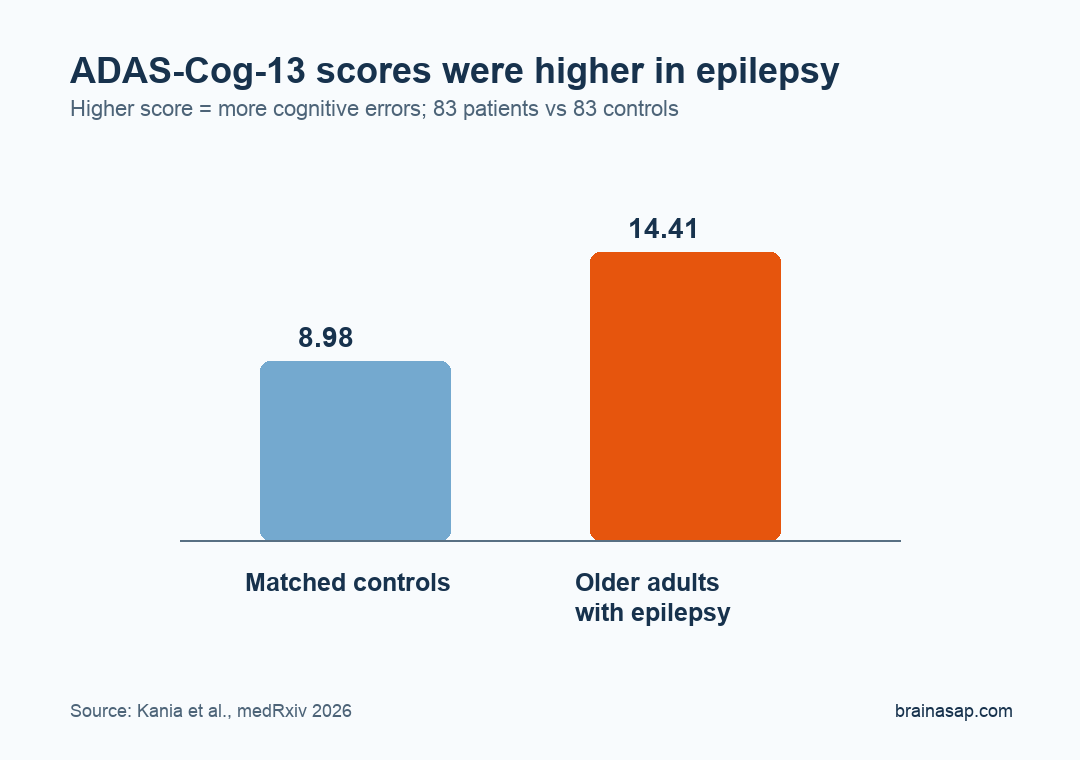
- Total scores were worse: Epilepsy participants had higher, more impaired ADAS-Cog-13 scores than controls, 14.41 versus 8.98.
- Memory items led the difference: The largest effects were on word recall (d = 0.87) and delayed word recall (d = 1.06).
- Cutoff 15 was modest: An ADAS-Cog-13 score of 15 or higher classified IC-CoDE impairment with 67.5% accuracy, 68.8% sensitivity, and 66.7% specificity.
Source: medRxiv (2026) | Kania et al.
Alzheimer’s Disease Assessment Scale-Cognitive Subscale 13-item version (ADAS-Cog-13) is widely used in Alzheimer’s disease and mild cognitive impairment research. This study asked whether the same scale can help screen older adults with epilepsy, a group with elevated cognitive and dementia-related risk.
The need is practical. Older adults are a growing share of epilepsy care, and cognitive screening is still inconsistent even though memory, language, processing speed, and daily function can be affected by seizures, brain aging, medications, and comorbid disease.
ADAS-Cog-13 Was Tested Against an Epilepsy Cognitive Standard
The epilepsy sample came from the Brain, Aging, and Cognition in Epilepsy (BrACE) cohort, a multicenter study of older adults with focal epilepsy. Participants were at least 55, English-speaking, and had no dementia diagnosis at enrollment.
Controls came from the Alzheimer Disease Neuroimaging Initiative (ADNI-3), a major aging and dementia research cohort. Researchers matched each epilepsy participant to one cognitively healthy control by age, sex, and education.
- Epilepsy group: 83 older adults with focal epilepsy, mean age 66.4 years.
- Control group: 83 cognitively healthy ADNI-3 participants matched 1:1 to the epilepsy group.
- Clinical benchmark: The International Classification of Cognitive Disorders in Epilepsy (IC-CoDE), which classifies impairment across domains such as memory, language, processing speed, attention, and executive function.
The ADAS-Cog-13 takes about 25 to 35 minutes and scores errors across tasks. Higher scores mean worse performance, so the epilepsy group’s higher average score represented more impairment.
Older Adults With Epilepsy Scored Worse on Memory and Language Items
Compared with controls, epilepsy participants had a higher total ADAS-Cog-13 score: 14.41 versus 8.98. The effect size was large, with d = 1.12 for the total-score difference.
Eight of the 13 individual test items differed significantly between groups. The strongest differences were concentrated in verbal learning and memory rather than every cognitive task.
- Word recall: Epilepsy participants performed worse, with effect size d = 0.87.
- Delayed word recall: The largest item difference was delayed recall, with d = 1.06.
- Word finding: Word-finding difficulty also differed, with d = 0.56.
- Unaffected items: Commands, constructional praxis, ideational praxis, orientation, and spontaneous spoken language were comparable across groups.
The memory-heavy pattern fits focal epilepsy in older adults, especially when temporal-lobe networks are involved. It also explains why a dementia-trial scale might detect impairment even outside a diagnosed Alzheimer’s disease sample.
An ADAS-Cog-13 Cutoff of 15 Had Modest Screening Accuracy
Within the epilepsy cohort, 32 of 83 participants, or 38.6%, were classified as cognitively impaired by IC-CoDE. Memory was the most common affected domain, followed by language and attention/processing speed.
Researchers tested ADAS-Cog-13 cutoffs from 14 to 18 to see which threshold best matched IC-CoDE impairment. A score of 15 or higher produced the best overall balance.
- Accuracy: 67.5% of participants were classified correctly against IC-CoDE.
- Sensitivity: 68.8% of IC-CoDE-impaired participants were detected by the cutoff.
- Specificity: 66.7% of IC-CoDE-intact participants were correctly classified as not impaired.
- AUC: The area under the receiver operating curve was 0.677, a modest discrimination result.
Those numbers support ADAS-Cog-13 as a screening option, not a diagnostic replacement for full neuropsychological testing. A cutoff that misses about one-third of impaired participants and falsely flags about one-third of intact participants needs follow-up assessment.
MoCA Performed Better, but ADAS-Cog May Track Memory Risk Differently
The study also compared ADAS-Cog-13 with the Montreal Cognitive Assessment (MoCA), a brief cognitive screen used in many clinics. MoCA showed higher overall classification accuracy and a higher area-under-the-curve value in this cohort.
The two tools have different roles. MoCA is shorter and easier to deploy during routine clinic visits.
ADAS-Cog-13 gives more detailed memory and language information. It is also already embedded in Alzheimer’s disease clinical-trial research, which may help epilepsy studies track neurodegenerative risk.
- Clinic screening: MoCA may remain the more efficient first screen for many epilepsy clinics.
- Research alignment: ADAS-Cog-13 may help connect epilepsy cognitive studies with Alzheimer’s and mild-cognitive-impairment trials.
- Memory emphasis: The delayed-recall signal may fit studies that specifically track memory vulnerability in older focal epilepsy.
The study was also cross-sectional. It cannot show whether an ADAS-Cog-13 score of 15 predicts future dementia, biomarker positivity, or faster cognitive decline in epilepsy.
Longitudinal follow-up with Alzheimer’s biomarkers would be needed before the cutoff could be treated as a dementia-risk marker.
The Finding Supports Referral Triage, Not Stand-Alone Diagnosis
For referral triage, ADAS-Cog-13 detected a meaningful cognitive difference between older adults with epilepsy and matched controls. It also roughly tracked IC-CoDE impairment inside the epilepsy cohort.
The sample was predominantly White, highly educated, and centered on focal epilepsies, which limits generalizability. The study was also a preprint, and it did not establish cross-cultural thresholds or language-specific performance.
For epilepsy care, the scale may work best as a structured reason to refer for full neuropsychological evaluation, especially when memory complaints, medication complexity, or dementia-risk concerns are already present.
Citation: DOI: 10.64898/2026.05.27.26354210. Kania et al. Utility of the ADAS-Cog as a Cognitive Screening Tool in Older Adults with Epilepsy: A Multicenter Cohort Study. medRxiv. 2026.
Study Design: Multicenter cohort analysis comparing older adults with focal epilepsy against matched healthy controls and IC-CoDE cognitive classifications.
Sample Size: 83 older adults with focal epilepsy and 83 matched cognitively healthy controls.
Key Statistic: ADAS-Cog-13 total score of 15 or higher identified IC-CoDE impairment with 67.5% accuracy, 68.8% sensitivity, and 66.7% specificity.
Caveat: The study was cross-sectional and preprint-stage, and the cutoff needs longitudinal and more diverse validation.