
TL;DR: A 2026 study in Computers in Human Behavior grouped 1,316 U.S. adults by when they first saw sexually explicit media and when regular viewing began; the highest distress appeared in people who moved into regular viewing early, while late regular engagement looked lower-risk in this cross-sectional survey.
Key Findings
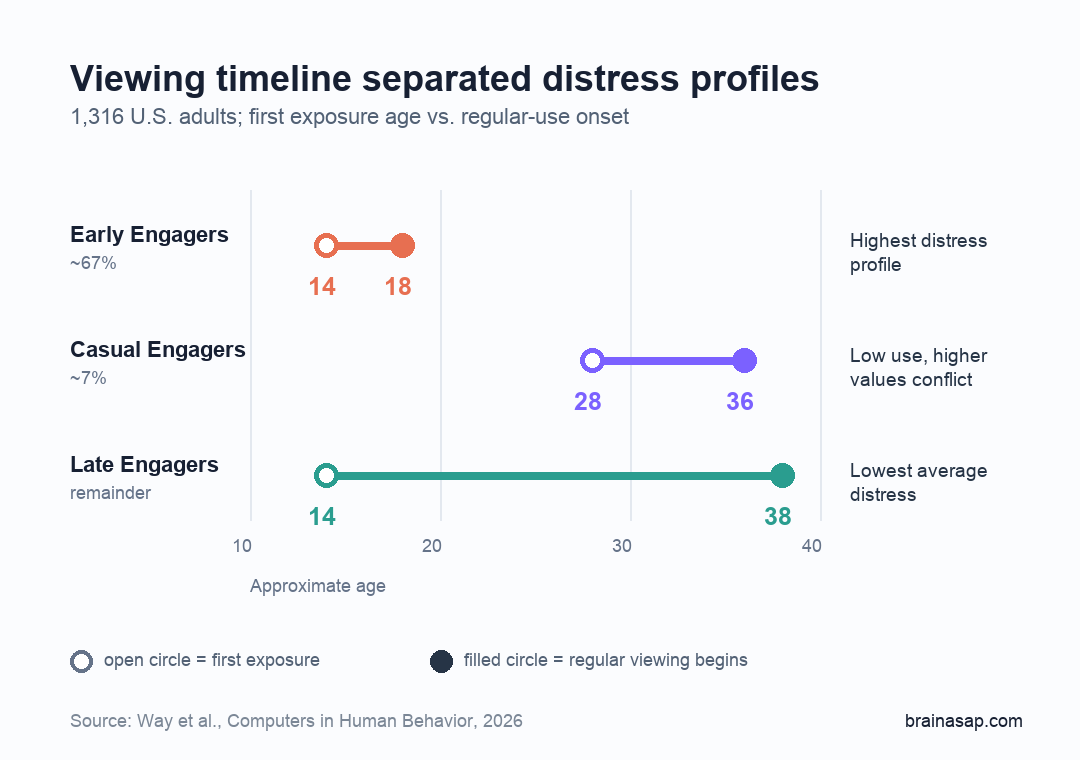
- Three trajectories emerged: researchers identified Early Engagers, Casual Engagers, and Late Engagers based on exposure age and regular-use age.
- Early Engagers were most common: about 67% of the sample first saw adult content around age 14 and began regular viewing around age 18.
- Distress was profile-specific: Early Engagers reported more depression, anxiety, suicidal ideation, and other risk behaviors, while Casual Engagers had low use but still reported distress tied to conflict with values.
- Late regular use looked lower-risk: Late Engagers also reported early exposure, but they did not begin regular viewing until around age 38.
- Causation remains unresolved: the survey design links profiles with distress, but it cannot prove that viewing timeline caused later symptoms.
Source: Way et al. Computers in Human Behavior. 2026.
Timing of Regular Viewing Mattered More Than First Exposure
Researchers analyzed whether the timeline of sexually explicit media use explained risk more clearly than first exposure alone. Many people first encounter adult content accidentally or passively, especially online.
The more clinically relevant point is when viewing becomes regular, intentional, and repeated.
The study used survey data from 1,316 American adults and asked two timing items: when participants first saw sexually explicit material and when they first began viewing it regularly.
Researchers then used latent profile analysis, a statistical grouping method that looks for shared patterns inside a dataset, to sort people by their developmental timeline.
The three profiles separated exposure from routine use:
- Early Engagers: first exposure around age 14, regular viewing around age 18, and the highest current viewing frequency.
- Casual Engagers: first exposure around age 28, regular viewing around age 36, and the lowest current use.
- Late Engagers: first exposure around age 14, but regular viewing did not begin until around age 38.
The group split changes how the result should be read. Early exposure by itself did not define the highest-risk group. The lower-distress Late Engagers also reported early first exposure.
What separated them was timing. They did not move quickly into regular viewing, so the strongest marker was the early transition from exposure to regular engagement.
Early Engagers Had the Highest Distress and Risk-Behavior Scores
Early Engagers made up the largest group, roughly two-thirds of the sample. Compared with the other profiles, they reported more frequent current viewing, longer sessions, and more signs of problematic use.
In clinical terms, problematic use means the behavior is harder to control, creates distress, or interferes with daily functioning.
The mental-health pattern was broader than viewing frequency. Early Engagers scored higher on screeners for depression, anxiety, and suicidal ideation.
They also reported more symptoms related to alcohol use, cannabis use, and gambling. The survey cannot prove that early regular viewing caused those outcomes, but the clustering suggests that timing may mark a wider vulnerability profile.
The results fit a familiar pattern from addiction and behavioral-risk research:
- Earlier routine engagement: a behavior becomes part of daily life while self-control systems and coping habits are still developing.
- Higher intensity: repeated use may be linked with longer sessions, more frequent viewing, or escalation into more intense content.
- More comorbidity: the same group may show higher distress and more substance-use or gambling symptoms.
Not every teenager who encounters adult content is on a fixed path. The comparison with Late Engagers argues against that simple interpretation.
The analysis instead highlights a more specific risk marker: how fast first exposure becomes regular use, and whether the behavior becomes tied to mood regulation or loss of control.
Low Use Was Not Always Low Distress
The Casual Engager profile adds an important caveat. This was the smallest group, about 7% of participants, and it had the lowest current viewing.
Yet Casual Engagers still reported depression and anxiety symptoms at levels closer to Early Engagers than to Late Engagers.
Researchers linked the Casual Engager result to moral incongruence, which means a behavior conflicts with a person’s religious, moral, or personal values.
In that situation, the distress may come less from frequency and more from interpretation. A rare behavior can feel severe if it violates a deeply held identity or belief system.
Clinicians need that distinction because two people can report distress for different reasons:
- Loss-of-control distress: viewing feels compulsive, hard to stop, or disruptive to relationships and work.
- Values-conflict distress: viewing is infrequent, but the person experiences guilt, shame, or anxiety because it conflicts with beliefs.
- Mixed distress: the behavior is both frequent and values-conflicting, which may need a different treatment conversation.
A one-size screening question about frequency would miss that difference. The study suggests that assessment should ask about timing, control, distress, and values, not just how often someone views sexually explicit media.
The Survey Design Cannot Prove Cause and Effect
The strongest limitation is causality. This was a cross-sectional survey, meaning all measures were collected at one point in time.
Researchers could identify profiles and associations, but they could not determine whether early regular viewing caused later mental-health symptoms.
The reverse path is also plausible. Some adolescents with early anxiety, depression, loneliness, or identity stress may use adult content as a coping tool.
If that behavior temporarily reduces negative emotion, it can become more regular. The viewing timeline could then be a marker of earlier distress rather than the original cause.
Memory is another limitation. Adults were asked to recall ages of first exposure and first regular viewing, sometimes from many years earlier.
Retrospective recall can be imprecise, and technology access differed sharply across generations. Older adults did not have the same smartphone and broadband environment that shaped younger participants’ exposure.
Clinical Screening Should Ask About the Timeline
The practical takeaway is not that first exposure alone predicts future mental health. A more useful screening frame is developmental: when did exposure happen, when did regular viewing begin, and what role does the behavior play now?
For mental-health assessment, four details are useful:
- First exposure: how old was the person when sexually explicit media first appeared?
- Regular-use onset: when did viewing become intentional and repeated?
- Current function: does viewing involve craving, failed control attempts, distress, or interference?
- Meaning and values: does distress come from behavior intensity, values conflict, or both?
Those details keep the interpretation narrow. The study does not label all adult-content viewing as pathological.
It shows that developmental timing and psychological context can separate very different risk profiles inside the same broad behavior.
Citation: DOI: 10.1016/j.chb.2026.108905. Way et al. Early exposure and emerging risk: A latent profile analysis of pornography use trajectories and their psychological correlates. Computers in Human Behavior. 2026.
Study Design: Cross-sectional survey with latent profile analysis.
Sample Size: 1,316 U.S. adults.
Key Statistic: Early Engagers made up about 67% of the sample and reported the highest psychological distress profile.
Caveat: The survey is observational and retrospective, so it cannot prove that early regular viewing caused later mental-health symptoms.





