TL;DR: A 2026 paper in Current Therapeutic Research described an acute PGAD-like genital arousal episode after self-initiated duloxetine withdrawal, with symptoms resolving within 5 hours after emergency admission and no recurrence over 36 months.
Key Findings
- 59-year-old patient: The case involved a woman with multiple sclerosis, fibromyalgia, restless legs syndrome, overactive bladder, and mixed anxiety-depressive disorder.
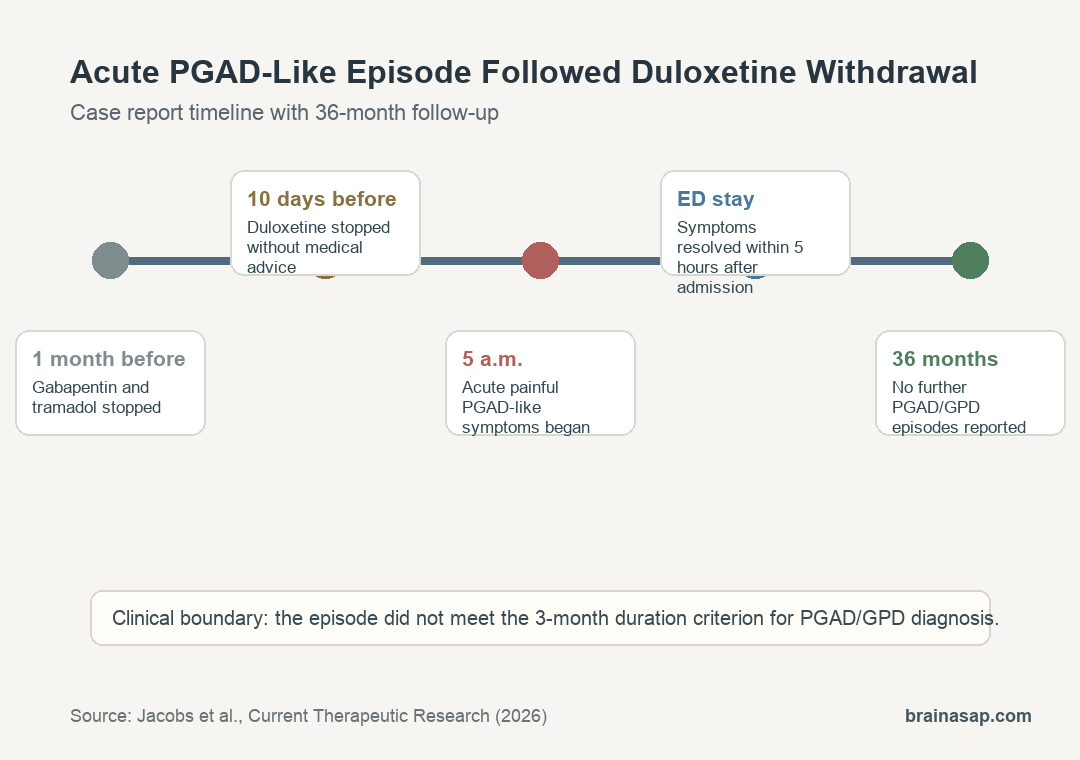
- Duloxetine stopped 10 days before: The serotonin-norepinephrine reuptake inhibitor was discontinued without prior medical advice.
- Symptoms began at 5 a.m.: The episode involved painful unwanted genital arousal symptoms without sexual thoughts or physical stimulation.
- 5-hour resolution: Symptoms resolved spontaneously within 5 hours after emergency admission, before intravenous amitriptyline and clorazepate were started.
- 36-month follow-up: The patient remained free of further PGAD/GPD episodes during follow-up.
Source: Current Therapeutic Research (2026) | Jacobs et al.
Acute PGAD-Like Symptoms Followed Recent Duloxetine Withdrawal
Persistent genital arousal disorder/genito-pelvic dysesthesia (PGAD/GPD) describes unwanted, intrusive, distressing genital arousal sensations that are not driven by sexual desire.
The Jacobs case did not meet the full duration criterion for PGAD/GPD because it was a first episode and did not persist for at least 3 months.
The duration boundary is central. The report described an acute PGAD-like episode, not a confirmed chronic PGAD/GPD diagnosis.
The ISSWSH consensus criteria also emphasize distress, unwanted sensations, and the absence of ordinary sexual desire as part of the clinical picture. This patient matched those features during the emergency visit.
The patient had several possible risk factors, including multiple sclerosis, restless legs syndrome, overactive bladder, fibromyalgia, sleep apnea, chronic fatigue syndrome, and mixed anxiety-depressive disorder.
The medication timeline made duloxetine withdrawal the leading suspected contributor. Gabapentin and tramadol had been stopped about 1 month earlier, while duloxetine was stopped 10 days before symptom onset.
Emergency Assessment Found No Pelvic Mass or Infection
The episode began at 5 a.m. during sleep. The patient reported painful genital symptoms, intense distress, shame about seeking care, and no sexual thoughts or physical stimulation.
Emergency assessment did not find a simple local explanation. Vital signs were normal, the abdominal exam was nonspecific, and pelvic examination did not reduce or provoke symptoms.
The team also reported no visible genital arousal, a negative urine dipstick test, and pelvic ultrasound that ruled out pelvic congestion syndrome.
- Local pelvic screen: no pelvic mass, dermatological disease, or ultrasound evidence of pelvic congestion syndrome.
- Medication review: recent duloxetine withdrawal stood out against longer-standing comorbidities.
- Specialist input: the gynecological surgery team sought pain-clinic expertise after the suspected diagnosis was made.
Symptoms Resolved Within 5 Hours After Admission
The episode was self-limited. Symptoms resolved spontaneously within 5 hours after admission and before intravenous amitriptyline and clorazepate were initiated.
Those medications were still introduced for ongoing pain and anxiety management, along with paracetamol and tramadol. The patient was discharged on day 1 with amitriptyline, paracetamol, and tramadol.
The regional drug-safety center reviewed the case and concluded that recent duloxetine cessation might be responsible for the acute PGAD-like episode. The case was registered in the national pharmacovigilance database.
The report also applied the Naranjo adverse drug reaction probability scale for withdrawal. Duloxetine discontinuation scored 6, corresponding to a probable adverse drug reaction.
That score did not settle causality. It organized the medication-history evidence so the withdrawal explanation could be weighed against neurological, bladder, pain, and sleep comorbidities.
36-Month Follow-Up Found No Further PGAD/GPD Episodes
Follow-up was unusually helpful for a case report. After 36 months, the patient remained symptom-free and reported no additional PGAD/GPD episodes.
Later evaluation did not reveal a better structural explanation. Pelvic MRI was normal for the uterus and ovaries and excluded sacral nerve root compression.
Brain and spinal MRI showed stable multiple-sclerosis-related findings and lumbar degenerative disc disease. That follow-up helped separate the new medication-timing clue from older neurological findings.
That does not prove duloxetine withdrawal caused the episode. It strengthens the temporal argument because alternative explanations were long-standing or stable, while duloxetine had been stopped shortly before the event.
- Most plausible trigger: self-initiated duloxetine discontinuation 10 days before symptom onset.
- Competing factors: multiple sclerosis, restless legs syndrome, overactive bladder, and other comorbidities could contribute to vulnerability.
- Clinical outcome: no recurrence was reported across 36 months.
Medication History Belongs in PGAD/GPD Assessment
The practical clinical lesson is medication history. PGAD/GPD literature includes pharmacological contributors, including starting or discontinuing SSRIs or SNRIs.
Duloxetine is an SNRI, a serotonin-norepinephrine reuptake inhibitor. In this case, the timing pointed toward withdrawal rather than ongoing exposure.
The report also highlights distress. PGAD/GPD symptoms can involve shame, pain, anxiety, and suicidality, so dismissive responses can delay care.
The emergency-team response is part of the clinical record. The patient sought care despite embarrassment because the distress was severe, and the team documented a workup rather than treating the complaint as nonmedical.
Three caveats are important:
- Single case: the report cannot estimate how often duloxetine withdrawal causes PGAD-like episodes.
- Acute episode: the symptoms did not satisfy the 3-month PGAD/GPD duration criterion.
- Multiple risk factors: comorbid neurological, bladder, pain, and sleep conditions complicate causal attribution.
Still, the case supports a careful rule for clinicians: when PGAD-like symptoms appear suddenly, recent antidepressant changes should be reviewed alongside pelvic, neurological, and psychological factors.
Citation: DOI: 10.1016/j.curtheres.2026.100823. Jacobs et al. Acute PGAD-Like Genital Arousal in a 59-Year-Old Woman After Duloxetine Withdrawal: A 36-Month Follow-Up Case Report. Current Therapeutic Research. 2026;104:100823.
Study Design: Single-patient case report with emergency assessment, pharmacovigilance review, imaging follow-up, and 36-month clinical follow-up.
Sample Size: 1 woman, age 59, with acute PGAD-like symptoms after recent medication discontinuation.
Key Statistic: Symptoms resolved spontaneously within 5 hours after admission, and no recurrence was reported during 36 months of follow-up.
Caveat: One acute case can support medication-history vigilance, but it cannot prove duloxetine withdrawal is a common or sufficient cause of PGAD/GPD.





