TL;DR: A 2026 electroencephalography (EEG) study in Cognitive, Affective, & Behavioral Neuroscience found that observers’ empathy-for-pain ratings and physiological coupling stayed similar whether they watched another person receive painful stimulation through a live video call or a prerecorded video, although live interaction produced an earlier frontal theta brain response.
Key Findings
- 35 observers tested: Researchers recruited 35 students; usable analysis samples were 31 for behavioral ratings, 31 for observing-condition EEG, 31 for skin conductance, and 32 for heart-rate timing.
- Live felt more immediate: Observers rated the video call as more immediate than the prerecorded condition, with t(29) = 5.16, p < .001, and d = 0.94.
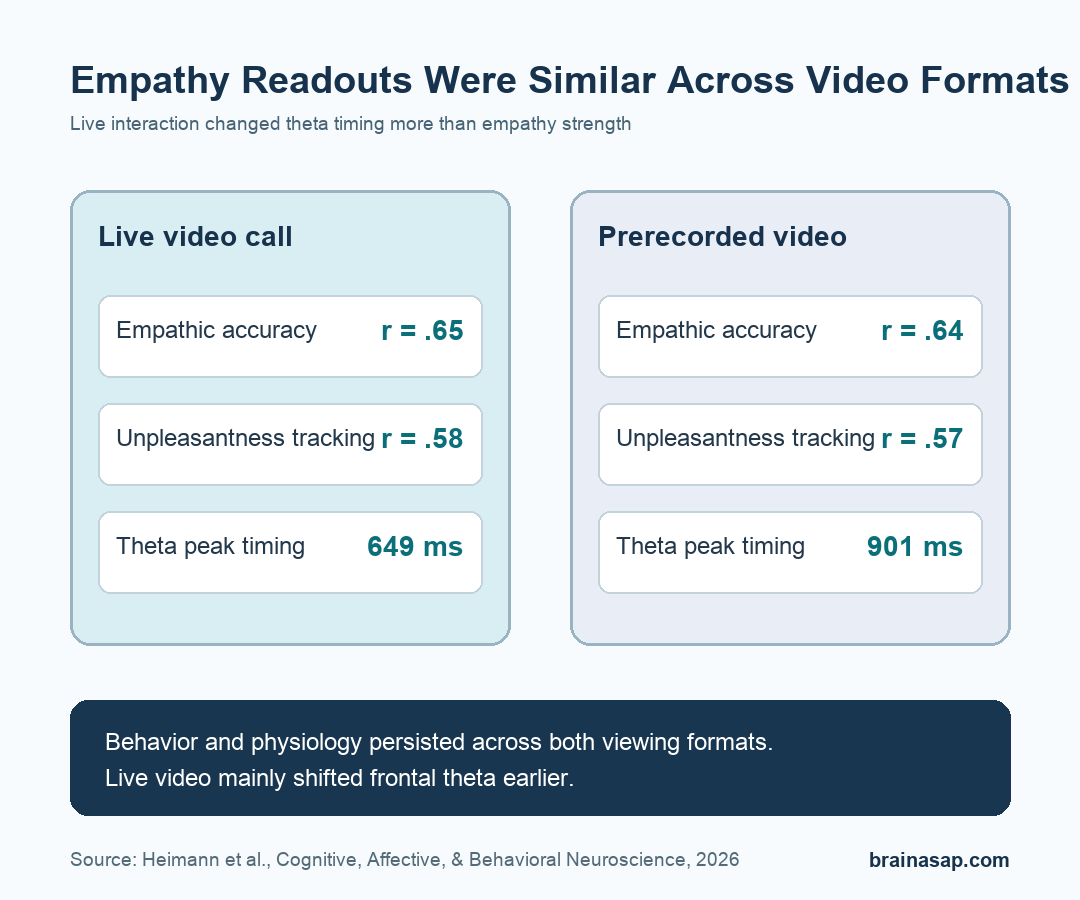
- Empathic accuracy stayed high: Observer and target pain ratings correlated almost identically in the video-call condition, r(31) = .65, and the prerecorded condition, r(31) = .64.
- Affective empathy also persisted: Observers’ unpleasantness ratings tracked targets’ pain ratings in both conditions, with correlations of r(31) = .58 for video call and r(31) = .57 for prerecorded video.
- Theta tracked observed pain: Frontal theta power increased with the target’s shock intensity, b = 0.12, p = .028, and the average theta peak occurred 252 ms earlier in the video-call condition.
Source: Cognitive, Affective, & Behavioral Neuroscience (2026) | Heimann et al.
Empathy for pain is not only a feeling report. Researchers treated it as a set of linked readouts: how accurately an observer judged another person’s pain, how unpleasant the observer felt while watching, and how the observer’s brain rhythms changed.
The analysis also asked whether the observer’s physiology moved with the target’s physiology.
The question was whether those readouts need live reciprocity. A live video call lets two people see each other in real time.
A prerecorded video keeps the same visual information about the target’s pain but removes immediate two-way social exchange.
Live Video Increased Immediacy But Did Not Increase Empathic Accuracy
Researchers designed the experiment so the social-presence manipulation was visible to participants. Observers reported that the video call felt more immediate and closer than the prerecorded video, while attachment to the other participant did not significantly differ.
The behavioral empathy result was not a failed manipulation. The live condition felt more live.
Empathic accuracy, meaning the match between the observer’s pain rating and the target’s own pain rating, stayed nearly the same across live and prerecorded viewing.
- Video-call accuracy: Observer and target pain ratings correlated at r = .65, with p < .001.
- Prerecorded accuracy: Observer and target pain ratings correlated at r = .64, also with p < .001.
- Rating distance: The average observer-target distance was small on a 0-100 visual analog scale: 1.99 points in video calls and -1.57 points in prerecorded videos.
The model comparison supported the same interpretation. The Bayes factor for adding condition to the empathic-accuracy model was BF10 = 0.001, which the researchers interpreted as extreme evidence against a meaningful condition effect.
Unpleasantness Ratings Followed The Target’s Pain In Both Conditions
The study separated cognitive and affective empathy. Cognitive empathy was represented by the observer’s estimate of the target’s pain.
Affective empathy was represented by the observer’s own unpleasantness while watching the target receive stimulation.
Observers’ unpleasantness ratings rose with the target’s pain ratings in both viewing formats. The video-call condition produced a slightly higher average unpleasantness rating, but the difference was only 1.66 points on the 0-100 scale, which the study treated as negligible.
- Video-call unpleasantness: Observers’ unpleasantness and targets’ pain correlated at r = .58.
- Prerecorded unpleasantness: The same relationship was r = .57.
- No interaction: The target-pain-by-condition interaction was not significant, p = .635, meaning the pain-to-unpleasantness relationship did not meaningfully change with temporal presence.
Put plainly, seeing another person hurt through a recording was enough to preserve the main behavioral empathy pattern in this controlled task.
Frontal Theta Reflected Observed Pain, While Mu Suppression Did Not
The EEG analysis focused on neural oscillations: rhythmic brain activity measured from the scalp.
The positive neural result involved frontal theta, a low-frequency pattern often studied in attention, salience, and cognitive-control contexts.
In the planned analysis, observers’ theta power increased with the target’s shock intensity. The fixed-effect estimate for intensity was b = 0.12, with p = .028.
Temporal presence itself was not significant, and the interaction between condition and shock intensity was also not significant.
Mu suppression, measured over the sensorimotor cortex in the 8-12 Hz range, did not show the expected sensitivity to the target’s pain intensity. Beta power also did not show a pain-intensity effect in the planned model.
- Theta: Target shock intensity predicted observer theta power, but condition did not.
- Mu: Target shock intensity did not significantly predict mu power, p = .280.
- Beta: Target shock intensity did not significantly predict beta power, p = .556.
An exploratory whole-time-frequency analysis sharpened the point. Observed pain was linked to a 1-6 Hz frontal theta cluster from 270 to 1,450 ms after shock onset.
A 9-13 Hz right posterior alpha decrease appeared from 870 to 1,550 ms. Neither condition nor the condition-by-intensity interaction survived correction.
Live Interaction Shifted Theta Timing By About 252 Milliseconds
The clearest difference was timing rather than overall strength. Exploratory latency analysis found that the theta peak arrived earlier when observers were in the live video-call condition.
The average frontal theta peak was 649 ms after shock onset in the video-call condition and 901 ms in the prerecorded condition. That 252 ms difference was statistically significant, t(30) = -2.78, p = .009, with Bonferroni-corrected p = .019.
Researchers checked whether this was just a technical timing artifact. The auditory N1 response to the sound cue peaked at 132 ms in the video-call condition and 141 ms in the prerecorded condition, which did not explain the larger theta latency difference.
- Strength was stable: Theta power did not meaningfully differ by live versus prerecorded viewing.
- Timing moved: Live interaction brought the peak theta response earlier.
- Interpretation stays cautious: The latency result was exploratory, so it should guide follow-up work rather than stand alone as a clinical claim.
Skin Conductance And Heart Timing Coupled Across Participants
Physiology added another layer. Researchers examined skin conductance response (SCR), a measure of sweat-gland-related autonomic arousal, and interbeat interval (IBI), the time between heartbeats.
Observers’ SCR was predicted by targets’ SCR, b = 0.15, p < .001. Observers’ IBI was also predicted by targets’ IBI, b = 1.71, p < .001. In both cases, condition did not meaningfully change the coupling.
- SCR coupling: The condition-by-target-SCR interaction was not significant, p = .861.
- IBI coupling: The condition-by-target-IBI interaction was not significant, p = .426.
- Practical meaning: In this lab task, autonomic alignment did not require a live reciprocal video connection.
This is narrower than saying recordings produce the same social experience as live interaction. The experiment tested a specific pain-observation task with controlled stimuli, not therapy, caregiving, conflict, or emotionally complex conversation.
The Result Narrows What Live Reciprocity Adds
The cleanest interpretation is that immediate two-way visibility may not be necessary for basic empathy-for-pain readouts when observers can clearly see another person’s pain expression and context.
The distinction is useful for digital social neuroscience, telehealth research, and online interaction debates because it separates two questions that often get blended together.
Live interaction can feel more immediate, and it may change neural timing, but some behavioral and physiological empathy markers can still survive without live reciprocity.
The limits are important:
- Small young sample: Participants were mainly university students, with usable samples near 31-32 people depending on the measure.
- Artificial pain task: Electric stimulation in a lab is controlled and measurable, but it is not the same as everyday social suffering or clinical pain.
- Low motivational stakes: Observers did not have to help the target, make a decision, or maintain an ongoing relationship.
- Exploratory timing result: The 252 ms theta-latency difference is useful, but it needs replication in more naturalistic settings.
For now, the study suggests a measured answer: prerecorded pain observation preserved several core empathy signals, while live video interaction mainly changed how quickly one EEG marker peaked.
Citation: DOI: 10.3758/s13415-026-01442-0. Heimann et al. Empathy for pain persists across live two-way video interactions and viewing of prerecorded videos. Cognitive, Affective, & Behavioral Neuroscience. 2026.
Study Design: Within-subject EEG and physiology experiment comparing live video-call pain observation with prerecorded pain-observation videos.
Sample Size: Thirty-five recruited students; usable analysis samples were 31 for behavior and observing-condition EEG, 31 for skin conductance, and 32 for heart-rate timing.
Key Statistic: Empathic accuracy correlations were nearly identical across conditions: r = .65 for video call and r = .64 for prerecorded video.
Caveat: The controlled lab task used a small young sample and may not capture empathy during real clinical, caregiving, or high-stakes social interactions.