TL;DR: A 2026 study in Drug and Alcohol Dependence Reports found 70 known Australian fatal poisonings involving new psychoactive stimulants and hallucinogens (NPSH), a category of newer stimulant- or hallucinogen-like drugs that often appeared alongside other psychoactive substances.
Key Findings
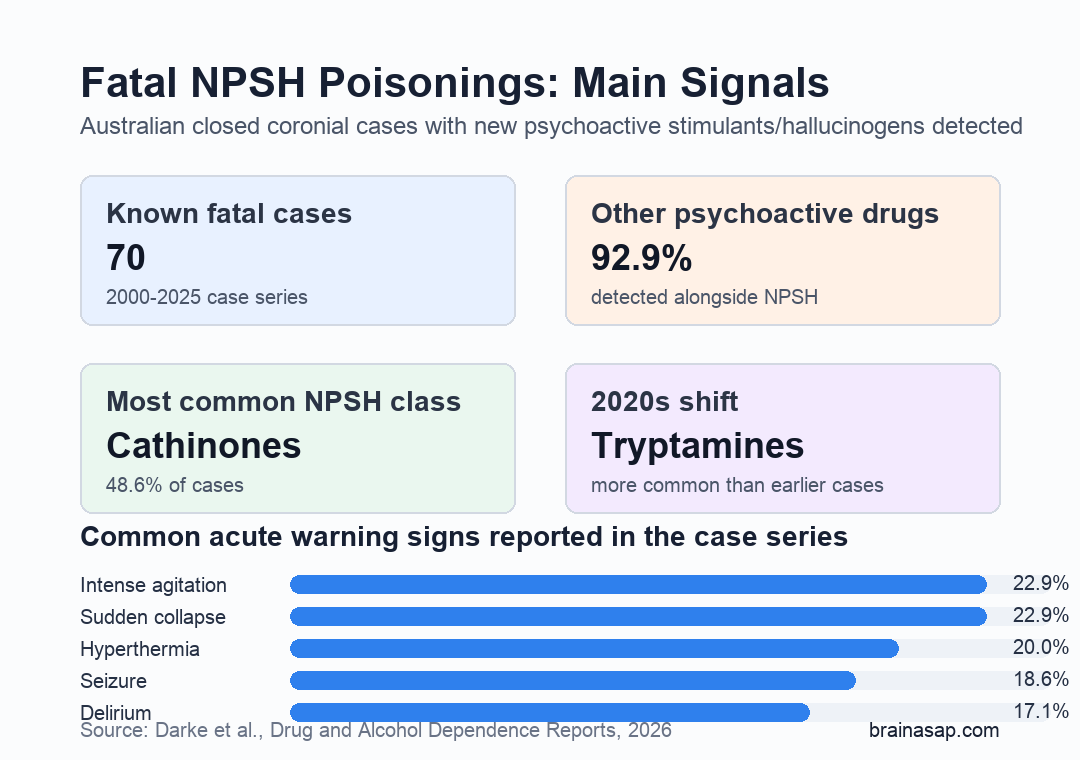
- Researchers identified 70 fatal drug-toxicity cases in Australia from 2000 to 2025 where NPSH were present in blood toxicology.
- Cathinones, a synthetic stimulant class, were the most common NPSH group, appearing in 48.6% of cases.
- Intense agitation, sudden collapse, hyperthermia, seizure, and delirium were the most common reported acute poisoning signs.
- 92.9% of cases also had other psychoactive drugs detected, most often other psychostimulants or hypnosedatives.
- Cases from the 2020s were more likely to involve tryptamines and less likely to involve phenethylamines than earlier cases.
Source: Darke et al. Drug and Alcohol Dependence Reports. 2026.
New psychoactive stimulants and hallucinogens are sometimes described as “designer drugs,” but that label can make the risk sound abstract. In this paper, the measured outcome was concrete: closed coronial cases where death was attributed to drug toxicity and blood toxicology detected an NPSH.
Researchers used the National Coronial Information System to identify fatal poisonings in Australia. The first case occurred in 2007, and 30 of the 70 cases occurred in the 2020s.
Fatal NPSH Poisonings Often Involved Multiple Drugs
The clearest public-health result was that these deaths rarely involved an isolated drug exposure. In 59 of 70 cases, the direct cause of death was multiple-drug toxicity rather than NPSH toxicity alone.
Blood toxicology showed a broad pattern of combined stimulant and hallucinogen exposure:
- Any other psychoactive drug: detected in 92.9% of cases.
- Other psychostimulants: detected in 68.6% of cases.
- Hypnosedatives: detected in 40.0% of cases.
- Multiple stimulants or hallucinogens: detected in 75.7% of cases.
Clinically, multiple stimulant or hallucinogen exposures can increase cardiovascular and neurotoxic stress. The paper describes this as a likely risk pattern for arrhythmias, cardiac arrest, seizures, and other acute toxicity events.
Cathinones Were the Most Common NPSH Class
Researchers identified 31 different NPSH across the case series. Thirteen were first detected in the 2020s, which fits the paper’s broader point that this drug market changes quickly.
The main NPSH classes were not evenly represented:
- Cathinones: present in 48.6% of cases, especially alpha-PVP and methylenedioxypyrovalerone (MDPV).
- Phenethylamines: present in 38.6%, including PMMA and NBOMe compounds.
- Tryptamines: present in 18.6%, most often DMT or 5-MeO-DMT.
- Piperazines: present in only a few cases.
Cathinones are synthetic stimulants. Phenethylamines and tryptamines include compounds with stimulant, hallucinogenic, or mixed effects.
The important point is not the chemistry taxonomy by itself. Newer substances kept appearing in fatal cases, and several cases involved more than one NPSH at the same time.
In 18 cases, or 25.7%, more than one NPSH was detected in blood. Five cases involved more than one NPSH class.
Agitation, Hyperthermia, Seizure, and Collapse Were Warning Signs
Signs and symptoms of acute poisoning were documented in 41 cases. The most common acute warning signs were intense agitation and sudden collapse, each reported in 22.9% of all cases.
Other common signs were hyperthermia, meaning dangerously high body temperature, in 20.0%; seizure in 18.6%; and delirium, a confused and disoriented mental state, in 17.1%.
The paper also reported common symptom pairings:
- Agitation plus delirium: reported together in 11 cases.
- Agitation plus hyperthermia: reported together in 8 cases.
- Agitation plus seizure: reported together in 7 cases.
- Hyperthermia plus seizure: reported together in 7 cases.
These are not subtle symptoms. The paper’s practical interpretation is direct: acute agitation, hyperthermia, seizure, delirium, and sudden collapse after suspected stimulant or hallucinogen use are medical-emergency signals, not “wait and see” events.
The 2020s Cases Showed a Shift Toward Tryptamines
The study compared deaths from the 2020s with earlier cases. Cases in the later period were older on average, but they did not differ clearly by sex, employment, documented substance-use history, injecting-drug history, mental-health history, or unintentional-death classification.
The more notable change was toxicology. Later cases were more likely to have tryptamines detected and less likely to have phenethylamines detected. Cathinone detection did not differ meaningfully between the periods.
This does not prove that tryptamines became more dangerous in a population-level sense. The paper studied known closed fatal cases, not total national exposure or all nonfatal poisonings.
Still, the shift supports toxicology surveillance that keeps pace with newer compounds rather than screening only for older drug classes.
Unrecognized Exposure Was Part of the Risk Pattern
In 16 cases, people present at the final drug consumption said the person had talked about using MDMA, methamphetamine, or LSD, but had not mentioned an NPSH. The paper interprets this as apparent unawareness that an NPSH was being consumed.
Several case characteristics make the prevention message practical:
- Unintentional deaths: 92.9% of cases were classified as unintentional.
- Private settings: most fatal incidents occurred in places such as a house, not at a music festival.
- Medical intervention: about half had ambulance or doctor involvement before death.
- Drug checking: the paper notes that buyers would be prudent to use drug-checking services where available.
The study does not argue that drug checking, emergency response, or toxicology screening can remove the risk. It does show why those measures matter: in many cases, the substance mix was broader than the person or bystanders appeared to understand.
Known Fatal Cases Are a Conservative Window Into the Problem
The main limitation is that the case series was based on closed coronial records and available toxicology. Recent cases may still be open, and some NPSH may not have been detected if laboratories were not testing for a newly emerging compound.
That means the study is best read as a profile of known fatal NPSH poisonings, not a complete national incidence estimate.
The result still gives clinicians and public-health teams a useful pattern: newer stimulants and hallucinogens appeared in fatal poisonings with frequent poly-drug exposure, rapidly changing drug classes, and acute warning signs that should trigger urgent medical care.
Citation: DOI: 10.1016/j.dadr.2026.100434. Darke et al. The toxicology and characteristics of fatal new psychoactive stimulant and hallucinogen-related poisonings in Australia, 2000-2025. Drug and Alcohol Dependence Reports. 2026;19:100434.
Study Design: Retrospective national coronial case series using Australian closed fatal drug-toxicity cases.
Sample Size: 70 fatal poisonings with NPSH detected in blood toxicology.
Key Statistic: Other psychoactive drugs were detected in 92.9% of cases, and cathinones were the most common NPSH class at 48.6%.
Caveat: Closed coronial cases and toxicology detection limits mean the case count is likely conservative and does not estimate total exposure risk.