TL;DR: A 2026 preprint posted to medRxiv found that intermittent theta-burst transcranial temporal interference stimulation (iTBS-tTIS), a noninvasive electrical method aimed at the right putamen, lowered left-sided Parkinson’s motor scores during stimulation in 19 patients.
Key Findings
- 19 Parkinson’s patients and 19 healthy controls completed a randomized, double-blind crossover stimulation study.
- MDS-UPDRS III, the motor section of a standard Parkinson’s clinical rating scale, improved more during real putamen-focused stimulation than during sham stimulation.
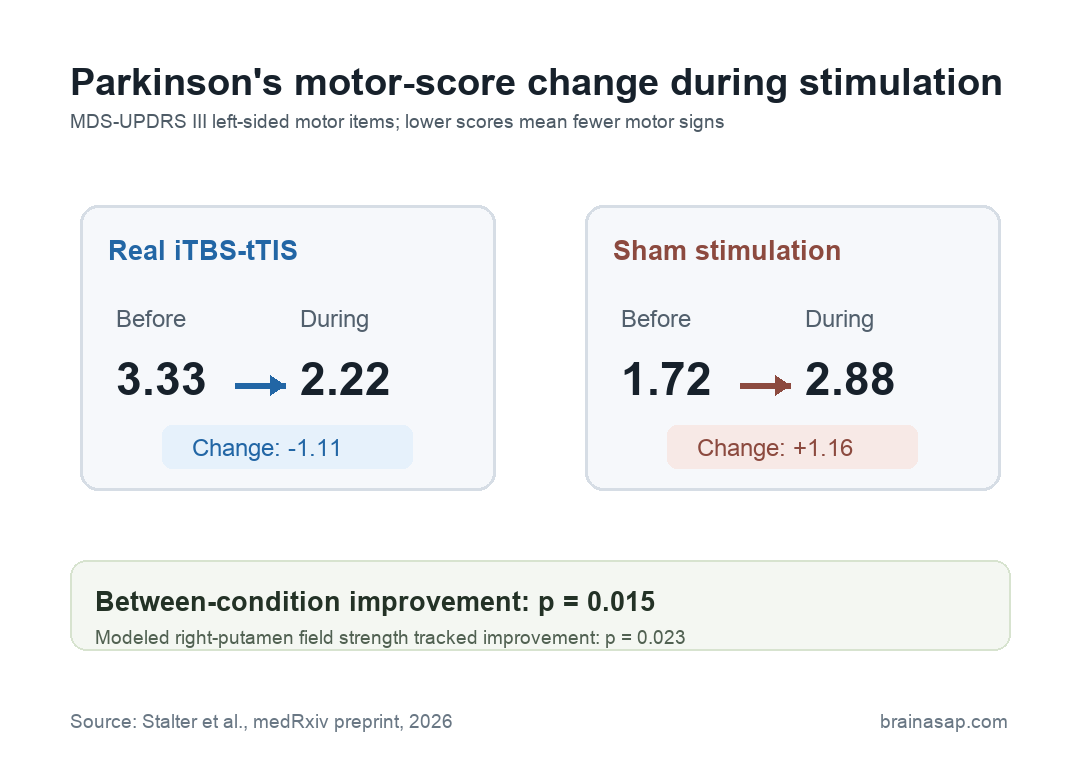
- Left-sided motor item scores changed by -1.11 points during stimulation versus +1.16 points during sham, with p = 0.015.
- Right-putamen electric field strength correlated with clinical motor-score improvement, suggesting that stronger modeled targeting tracked the short-term response.
- Tapping and motor-learning tasks did not show a reliable Parkinson’s benefit, and the preprint was not peer reviewed.
Source note: The study is a medRxiv preprint, so the finding should be treated as early clinical evidence rather than practice-changing proof.
Transcranial temporal interference stimulation tries to reach deep brain tissue without implanted electrodes.
Researchers apply two high-frequency currents from the scalp. Where the currents overlap, the difference between them creates a slower stimulation envelope in the target region.
In this trial, the target was the right putamen, a basal-ganglia structure involved in movement control. Parkinson’s disease affects basal-ganglia circuits, and the putamen is one of the main entry points into those motor loops.
Researchers used an intermittent theta-burst pattern, meaning short stimulation bursts were repeated with pauses. The stimulation was delivered while participants with Parkinson’s were in the medication ON state, meaning their usual Parkinson’s medication was active during testing.
Putamen-Focused tTIS Lowered Left-Sided Parkinson’s Motor Scores
The main clinical outcome was the Movement Disorder Society Unified Parkinson’s Disease Rating Scale Part III (MDS-UPDRS III), the motor-exam section of a widely used Parkinson’s rating scale.
Researchers focused on left-sided extremity items because stimulation was aimed at the right putamen, which is linked to movement control on the opposite side of the body.
The comparison was short-term and within person. Each participant went through both real stimulation and sham stimulation in a randomized, double-blind crossover design, with at least a 10-day washout between sessions.
- Real stimulation: Left-sided MDS-UPDRS motor items moved from 3.33 before stimulation to 2.22 during stimulation.
- Sham stimulation: The same left-sided score moved from 1.72 before sham to 2.88 during sham.
- Between-condition change: The real-versus-sham improvement was statistically significant at p = 0.015.
The design comparison is useful because the finding was not just a general before-and-after change. The preprint compared real stimulation against a sham condition inside the same participants, which makes the immediate clinical contrast more informative than a simple open-label test.
Modeled Putamen Field Strength Tracked Motor Improvement
Researchers also used each participant’s structural MRI scan to model how much electric field reached the right putamen. The average modeled field was similar in Parkinson’s patients and controls: 0.226 V/m in the Parkinson’s group and 0.242 V/m in healthy controls.
Within the Parkinson’s group, stronger modeled right-putamen field strength was linked to greater motor-score improvement. The correlation with MDS-UPDRS change reached p = 0.023.
Interpretation: The field-strength relationship supports the idea that the clinical change was connected to stimulation reaching the intended deep target. It does not prove durability, dose response, or long-term therapeutic value.
The targeting detail is important because noninvasive stimulation often faces a depth-versus-focality problem.
Stimulation that reaches deep brain regions can also affect overlying cortex, while more focal stimulation may not reach the desired circuit. tTIS is designed to reduce that tradeoff.
Tapping Tasks Did Not Show a Clear Parkinson’s Benefit
The motor-score result did not extend cleanly to every behavioral task. Researchers tested an alternating tapping task and a sequential finger tapping task to measure motor performance and motor learning.
- Alternating tapping: Healthy controls showed a stimulation effect, but researchers noted that it was likely driven by a lower baseline in one control-session condition.
- Parkinson’s tapping performance: The Parkinson’s group did not show a significant improvement on the alternating tapping task.
- Sequential finger tapping: No reliable real- or sham-stimulation benefit appeared in either group.
That split keeps the finding narrow. The most direct result was a short-term change in a clinical motor-exam score, not a broad improvement in learned finger-sequence performance.
Safety Findings Were Reassuring but Early
No severe side effects were reported. Mild events included fatigue, redness, concentration problems, dysesthesia, burning sensation, headache, local warming, neck pain, local pain, and one mood-change report.
Researchers described the mild side effects as mostly brief and roughly distributed between sham and active stimulation. Because the total event count was low, they did not run a formal statistical comparison of side-effect rates.
The safety finding is useful, but the sample was still small. A treatment approach meant for Parkinson’s symptoms would need larger studies, longer follow-up, repeated-session testing, and clearer dose-response data before it could be judged clinically.
Medication ON-State Testing Limits the Parkinson’s Claim
The Parkinson’s group was mildly to moderately affected. Their average MDS-UPDRS III score was 19.0, average disease duration was 6.26 years, and the average Hoehn and Yahr stage was 2.3.
Several limits shape the result:
- Small crossover sample: The Parkinson’s analysis included 19 patients, so the estimate needs replication.
- ON-state stimulation: Medication-active testing may have hidden or altered stimulation effects.
- Short stimulation window: The study measured online effects during stimulation, not sustained symptom change after treatment.
- Preprint status: The report had not completed peer review when posted.
Main takeaway: Putamen-focused iTBS-tTIS produced an immediate clinical motor-score improvement in this small Parkinson’s crossover trial, and modeled electric-field delivery to the putamen tracked that response.
Whether the method can produce meaningful, durable Parkinson’s symptom relief is still an open clinical question.
Citation: DOI: 10.64898/2026.02.05.26345627. Stalter et al. Intermittent Theta-burst Transcranial Temporal Interference Stimulation focusing on the Putamen improves Motor Functions in Parkinson’s Disease – A randomized, controlled Trial. medRxiv. 2026.
Study Design: Randomized, double-blind crossover preprint comparing real putamen-focused iTBS-tTIS with sham stimulation.
Sample Size: 19 Parkinson’s disease patients and 19 age- and sex-matched healthy controls.
Key Statistic: Left-sided MDS-UPDRS motor item change was -1.11 during real stimulation versus +1.16 during sham; p = 0.015.
Caveat: Small preprint study, medication ON-state testing, short stimulation exposure, and no durable motor-learning benefit.





