TL;DR: A 2026 scoping review in Nature and Science of Sleep found that sleep bruxism and gastroesophageal reflux disease were positively associated across 7 adult human studies, but the evidence remains too heterogeneous to prove causality.
Key Findings
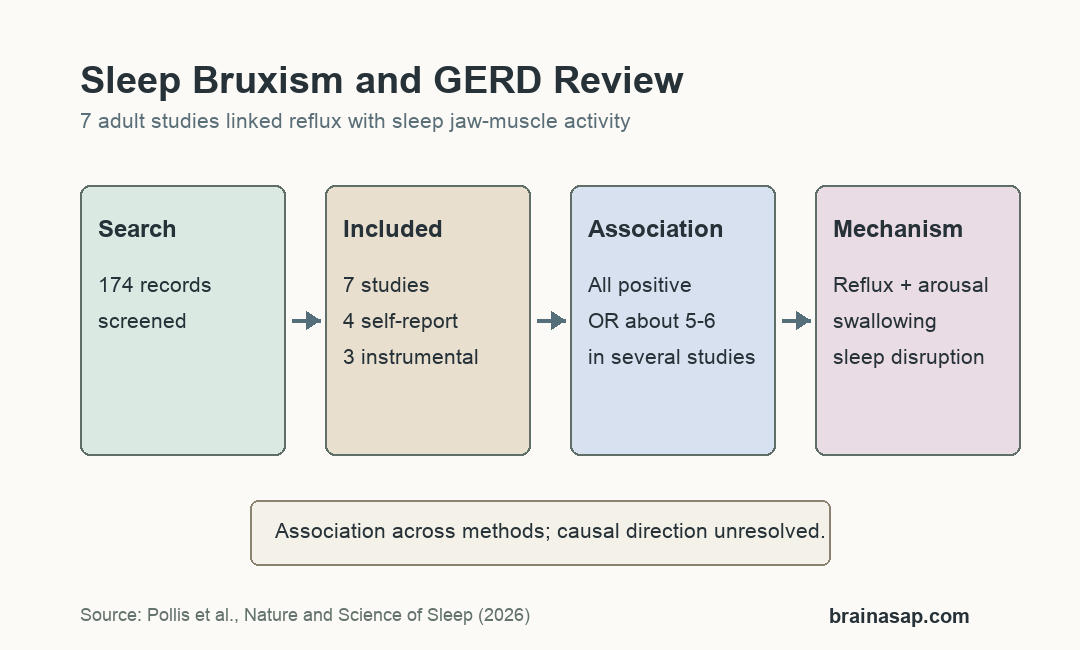
- 174 records screened: Database searches in PubMed, Scopus, and Web of Science narrowed 174 references to 7 included studies.
- 4 self-report/clinical studies: 4 studies used self-reported or clinical sleep-bruxism assessment, with total study populations above 2,800 participants.
- 3 instrumental studies: 3 studies used electromyography or polysomnography-based sleep-bruxism assessment, totaling 44 participants.
- 5- to 6-fold odds: Several observational comparisons found GERD associated with about 5- to 6-fold higher odds of sleep bruxism.
- PPI signal was mixed: 2 instrumental studies found proton pump inhibitor therapy reduced EMG bursts or rhythmic masticatory muscle activity, but effects were variable.
Source: Nature and Science of Sleep (2026) | Pollis et al.
Sleep Bruxism and GERD Were Reviewed as Overlapping Sleep Problems
Sleep bruxism means rhythmic or non-rhythmic jaw-muscle activity during sleep, including tooth grinding or clenching. It is no longer treated as a disorder in every person, because it can be harmless, damaging, or possibly protective depending on context.
Gastroesophageal reflux disease (GERD) involves stomach contents moving back into the esophagus and sometimes toward the throat or mouth. In sleep medicine and dental sleep medicine, reflux matters because it can disturb sleep, affect swallowing, and contribute to tooth erosion.
The review focused on adult human studies that measured the relationship between sleep bruxism and GERD. It excluded animal studies, case reports, preprints, reviews, and studies that did not supply clinical data on the relationship.
- Sleep-bruxism measures: self-report, clinical examination, electromyography (EMG), or polysomnography.
- GERD measures: questionnaires, endoscopy, or esophageal pH monitoring depending on the study.
- Main question: whether the 2 conditions co-occur and what mechanisms might connect reflux, arousals, swallowing, and jaw-muscle activity.
7 Studies Survived the Scoping Review Screen
The search identified 174 articles. After title, abstract, and full-text screening, 7 studies met inclusion criteria.
2 reviewers independently screened records and then charted the retained studies with a PECO-style structure: population, exposure, comparison, and outcome. That method helped separate study design, assessment approach, and relationship findings.
The included evidence split into 2 assessment groups. 4 studies used self-report or clinical sleep-bruxism assessment, while 3 used instrumental recording such as EMG or polysomnography.
- Self-report/clinical group: 4 studies, including 3 with clinical bruxism evaluation.
- Instrumental group: 3 studies using overnight EMG or polysomnography-style measurement.
- Evidence type: mostly observational and methodologically varied, which fits a scoping review better than a pooled meta-analysis.
GERD Was Associated With Higher Sleep-Bruxism Odds
All 4 self-report or clinical studies found a statistically significant relationship between sleep bruxism and GERD. 1 cross-sectional study reported a weak positive correlation between current sleep bruxism and GERD, with r = 0.112 and p = 0.044.
3 other observational studies reported larger odds-ratio estimates. GERD was associated with sleep bruxism at OR = 5.30, OR = 6.87, and OR = 6.58 in those comparisons.
The review summarized the observational evidence as roughly a 5- to 6-fold higher likelihood of sleep bruxism among patients with GERD compared with healthier comparison groups. That is a relationship signal, not proof that reflux alone causes tooth grinding.
- Weak correlation: 1 self-report study found r = 0.112, showing a small but statistically significant association.
- Higher odds: 3 studies found GERD-bruxism odds ratios between 5.30 and 6.87.
- Clinical caution: assessment differences make direct study-to-study comparison difficult.
Instrumental Studies Connected Reflux With Jaw-Muscle Activity
The instrumental studies were smaller, with 44 participants across the 3 included papers. They were important because EMG and polysomnography-style recordings can place jaw-muscle activity in time with sleep events or reflux measures.
In 1 study, the sleep-bruxism group had more gastroesophageal reflux episodes than controls. Another reported that rhythmic masticatory muscle activity and clenching episodes were more frequent during periods of lower esophageal pH.
2 studies also found that proton pump inhibitor therapy, a reflux-suppressing treatment, reduced EMG bursts or rhythmic masticatory muscle activity. The review treated this as supportive but not definitive because response varied and some jaw-muscle activity remained higher than healthy-control levels.
The instrumental evidence adds timing information because it moves beyond a patient saying they grind their teeth or have reflux symptoms. It still remains small, and it does not fully establish whether reflux happens first, jaw activity happens first, or both reflect the same arousal sequence.
Micro-Arousals May Link Reflux, Swallowing, and Bruxism
1 proposed mechanism is protective. Acid reflux during sleep can trigger arousal and swallowing, and jaw-muscle activity may help stimulate saliva or clear refluxed material.
Another proposed mechanism is shared sleep instability. Micro-arousals involve short shifts in brain activity and sympathetic activation, and rhythmic masticatory muscle activity can occur at the end of that arousal sequence.
- Protective hypothesis: jaw-muscle activity may support swallowing or salivation after reflux events.
- Arousal hypothesis: reflux, sleep fragmentation, and bruxism may cluster around micro-arousals.
- Sleep-quality hypothesis: anxiety, depression, and impaired sleep quality may partly mediate the relationship in some datasets.
The review’s main limitation is measurement heterogeneity. Future studies need standardized bruxism assessment, stronger GERD measurement, and better control for sleep apnea, psychiatric symptoms, medications, alcohol, smoking, and other sleep disorders.
For clinical readers, the finding supports asking about reflux symptoms when sleep bruxism is severe, new, or accompanied by tooth wear. It does not support treating every sleep-bruxism case as hidden GERD without a normal medical evaluation.
Citation: DOI: 10.2147/NSS.S574762. Pollis et al. Sleep Bruxism and Gastroesophageal Reflux. A Scoping Review. Nature and Science of Sleep. 2026;18:574762.
Study Design: Scoping review of adult human studies on sleep bruxism and gastroesophageal reflux disease.
Sample Size: 7 included studies after screening 174 records; 4 self-report/clinical studies and 3 instrumental studies.
Key Statistic: GERD was associated with sleep bruxism across all included studies, with several odds-ratio estimates around 5 to 6.
Caveat: Heterogeneous assessment methods and small instrumental studies prevent causal conclusions.