TL;DR: A 2026 medRxiv preprint enrolled 177 adults with migraine in a 30-day smartphone study and found that daily cognition and symptom check-ins were feasible, with 3,688 completed assessments and higher baseline burden in chronic migraine.
Key Findings
- Migraine cohort: The MIND study followed 177 adults with migraine using once-daily smartphone surveys and brief mobile cognitive tasks for 30 days.
- Daily monitoring held up: Participants completed 3,688 assessments, equal to 70.8% of all possible person-days.
- Most stayed engaged: 70.6% of participants completed at least 20 days of monitoring, and day-level completion stayed above 60%.
- Chronic migraine carried more burden: Chronic migraine was linked to higher MIDAS disability scores and more days with concentration difficulty and daily-life interference.
- Main caveat: The report is a preprint and feasibility/baseline cohort study, so it shows that the measurement approach works, not that smartphone monitoring improves migraine outcomes.
Source: Khorsand et al. 2026 medRxiv preprint.
Smartphone Monitoring Tried to Capture Migraine Brain Fog in Daily Life
Migraine is not only headache pain. Many people report brain fog, slowed thinking, trouble concentrating, sensory symptoms, fatigue, mood changes, and difficulty functioning before, during, or after headache days.
Traditional clinic visits can miss that day-to-day movement. A single cognitive test may not show whether attention drops before a migraine, whether poor sleep tracks with worse symptoms, or whether a treatment changes real-world cognitive function.
The Migraine Impact on Neurocognitive Dynamics study, or MIND study, tested a different approach. Researchers enrolled adults with migraine remotely and asked them to complete one smartphone-based assessment per day for 30 days.
The daily protocol combined ecological momentary assessment, meaning brief real-world surveys, with mobile cognitive tasks from the Mobile Monitoring of Cognitive Change battery.
- Symbol Search: A processing-speed and visual-scanning task.
- Color Dots: An attention and short-term memory task using color-location recall.
- Grid Memory: A visuospatial working-memory task using briefly shown grid patterns.
Each task was designed to take less than 2 minutes. A migraine monitoring tool has to be brief enough for repeated use on normal days, headache days, and days when fatigue or concentration problems are already present.
The 30-Day Protocol Reached 3,688 Daily Assessments
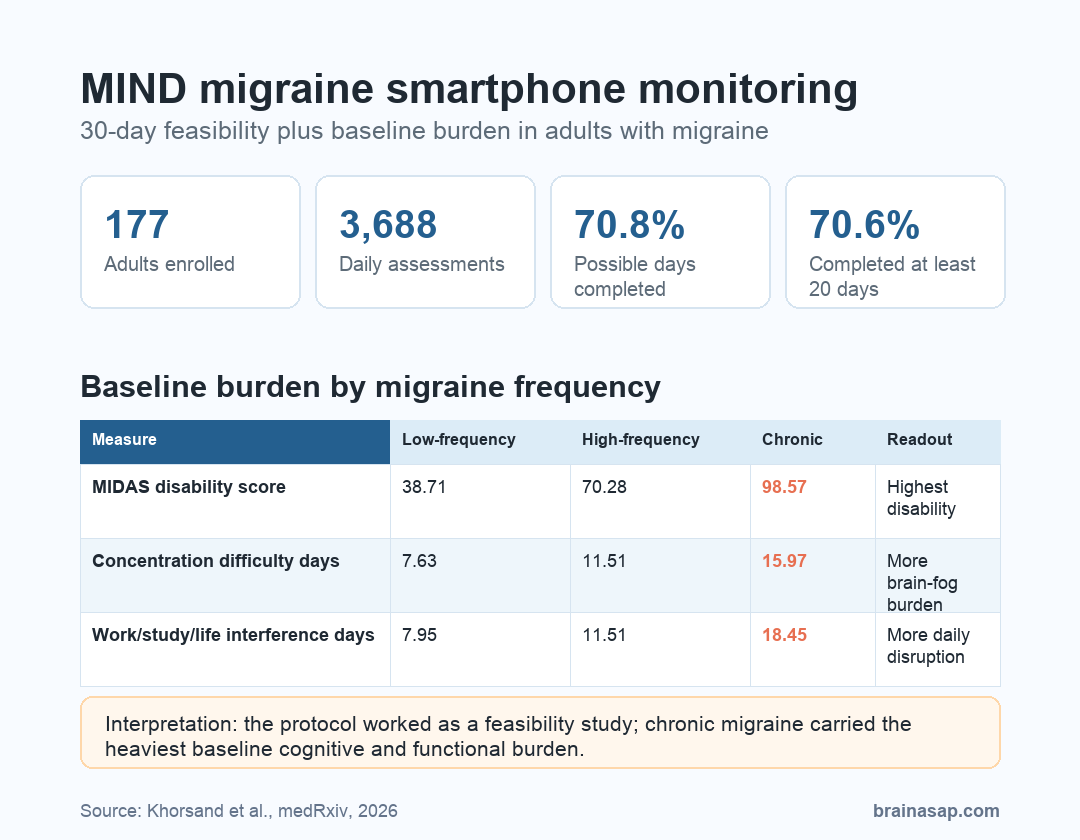
The final baseline cohort included 177 participants, with a mean age of 38.8 years. The sample was 79.7% female, and 80 participants, or 45.2%, had chronic migraine.
Across the 30-day protocol, participants completed 3,688 daily assessments. That represented 70.8% of all possible person-days, based on 177 people over 30 days.
Engagement was not limited to a small group of highly active users. 70.6% of participants completed at least 20 days of monitoring, and completion stayed above 60% across study days.
The timing data also suggest that participants often responded early in the daily window. Among completed surveys, 24.0% were filled out within the first hour, 53.9% within 4 hours, and 81.9% within 8 hours.
Missingness was low at the item level. Researchers reported that 27 of 29 daily assessment items had less than 2% total missingness.
Those higher-missingness items asked when headache started and which medications were taken that day.
Chronic Migraine Showed Higher Disability and Concentration Burden
The baseline results separated participants into low-frequency episodic migraine, high-frequency episodic migraine, and chronic migraine. The chronic migraine group had 15 or more migraine days per month.
Chronic migraine was associated with a heavier functional profile. The Migraine Disability Assessment Scale, or MIDAS, estimates headache-related disability over recent months.
Mean MIDAS scores were 38.71 in low-frequency episodic migraine, 70.28 in high-frequency episodic migraine, and 98.57 in chronic migraine.
The concentration measure moved in the same direction. Participants with chronic migraine reported 15.97 days with concentration difficulty, compared with 11.51 days in high-frequency episodic migraine and 7.63 days in low-frequency episodic migraine.
Daily-life interference also increased with migraine frequency. Chronic migraine participants reported 18.45 days when migraine interfered with work, study, or life, compared with 11.51 in the high-frequency episodic group and 7.95 in the low-frequency episodic group.
- Disability: MIDAS scores were highest in chronic migraine.
- Concentration: Reported concentration-difficulty days rose with migraine frequency.
- Function: Work, study, and daily-life interference was greatest in chronic migraine.
- Mood symptoms: PHQ-4 scores, a brief anxiety/depression symptom screen, were higher in chronic migraine than low-frequency episodic migraine.
Completion Was Lower When Brain Fog and Headache Days Were Higher
Completion was not equally easy for every participant. Completion rate had modest associations with several baseline or daily-experience variables.
Completion was lower among participants with higher subjective brain-fog severity, with r = -0.28 and p < 0.001. It was also lower when participants had a higher proportion of headache days, with r = -0.23 and p = 0.004.
Sleep quality went in the opposite direction. Better sleep quality was associated with higher completion, with r = 0.21 and p = 0.010.
- Measurement burden matters: The people with worse brain fog may be the same people least able to complete daily cognitive tasks consistently.
- Symptom timing matters: Headache days can affect whether a person opens the app, completes the task, or skips a day.
- Missingness is informative: In this kind of study, missed entries may partly reflect the condition being measured.
This missingness signal is important for future digital-health studies. A high adherence average can still hide symptom-linked missingness, and the missing days may carry clinical meaning.
The Useful Result Is Feasibility, Not Treatment Effect
The strongest conclusion is practical: a month-long smartphone protocol for migraine symptoms and brief cognitive testing can work at meaningful scale.
The result does not show that smartphone monitoring treats migraine, prevents brain fog, or replaces clinical evaluation. The study enrolled a digital cohort, used self-reported baseline measures, and reported feasibility plus baseline characteristics.
The next scientific step is within-person analysis. If daily cognitive scores, sleep, headache timing, medication use, and functional interference can be modeled together, researchers can ask whether cognitive changes appear before headache, during attacks, during postdrome, or between attacks.
- Protocol boundary: The preprint tested measurement feasibility and baseline burden.
- Clinical boundary: It should not guide treatment decisions without outcome studies.
- Research value: The design could help future migraine studies track brain fog and symptoms as moving daily states rather than static clinic snapshots.
The practical takeaway is specific. Migraine-related cognition is measurable outside the clinic, but the highest-symptom cases may also be the most likely to miss app-based assessments when symptoms are high.
Citation: DOI: 10.64898/2026.04.14.26350866. Khorsand et al. The MIND Study: Design, Feasibility, and Baseline Characteristics of a Smartphone-Based Migraine Cohort. medRxiv. 2026.
Study Design: Decentralized 30-day smartphone-based cohort feasibility and baseline-characteristics study.
Sample Size: 177 adults with migraine; 80 participants had chronic migraine.
Key Statistic: Participants completed 3,688 daily assessments, representing 70.8% of all possible study days.
Caveat: This is a preprint feasibility study, so it supports the measurement approach but does not establish clinical benefit from monitoring.