
TL;DR: A 2026 study in BJGP Open found no clear cohort-level increase in major bleeding outcomes when selective serotonin reuptake inhibitors (SSRIs) were used with direct oral anticoagulants (DOACs), but the self-controlled analysis still pointed to extra caution when an SSRI is newly started during DOAC treatment.
Key Findings
- No cohort increase: DOAC plus SSRI use did not show higher intracranial, gastrointestinal, or other bleeding risk than DOAC plus non-SSRI antidepressant use after propensity-score weighting.
- Large primary-care dataset: Researchers studied 35,782 DOAC+SSRI users and 39,745 DOAC+non-SSRI antidepressant users in UK CPRD Aurum records from 2011 to 2021.
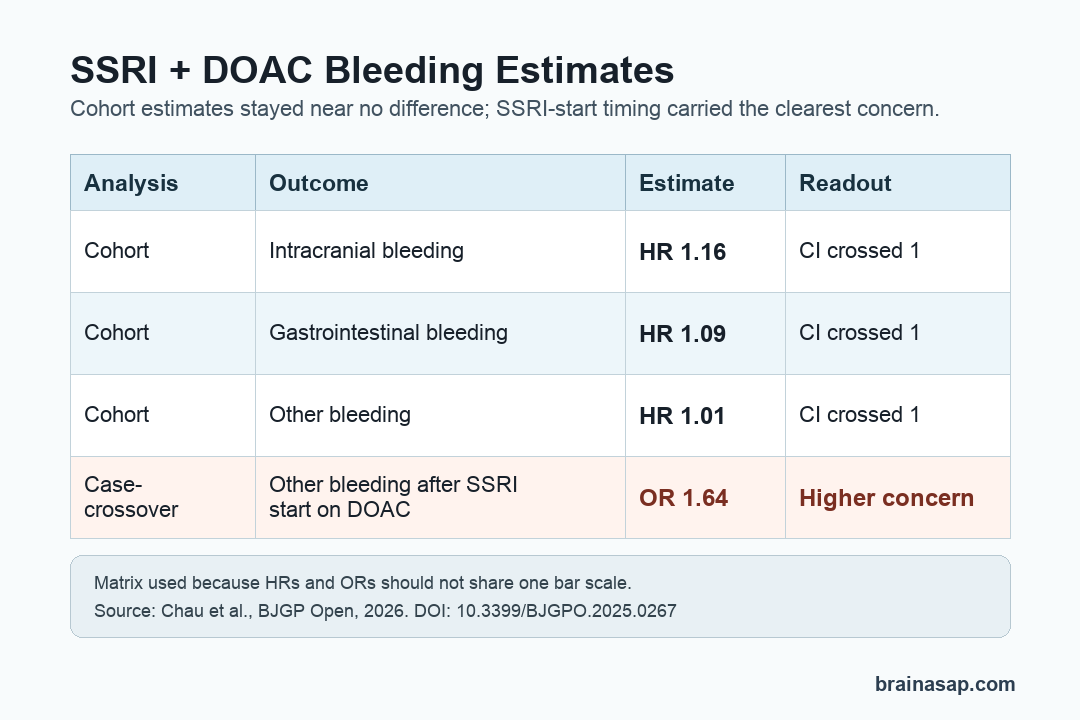
- Main hazard ratios stayed near 1: Intracranial bleeding was HR 1.16, gastrointestinal bleeding was HR 1.09, and other bleeding was HR 1.01, all with 99% confidence intervals crossing no difference.
- Initiation timing mattered: In the case-crossover analysis, starting an SSRI while already taking a DOAC was linked to higher odds of other bleeding (OR 1.64) than SSRI monotherapy.
- Clinical reading: The study supports careful monitoring at medication changes rather than a blanket conclusion that SSRI+DOAC use sharply raises major bleeding risk.
Source: BJGP Open (2026) | Chau et al.
The clinical issue sits at the overlap of mental-health treatment and clot prevention. An antidepressant choice can matter differently when a patient is also taking long-term anticoagulation.
The safety concern is straightforward: SSRIs can reduce platelet serotonin, which may weaken platelet aggregation, while DOACs already increase bleeding risk by blocking clotting pathways. Patients with stroke, atrial fibrillation, venous thromboembolism, depression, or anxiety can easily end up needing both drug classes.
Researchers Compared SSRI Users With Non-SSRI Antidepressant Users
Researchers used UK Clinical Practice Research Datalink (CPRD) Aurum primary-care records, linked hospital data, death registration data, and deprivation measures. The cohort covered adults who received a first DOAC prescription between January 1, 2011 and March 29, 2021.
The comparison was not SSRI users versus people with no antidepressant.
Instead, the main cohort analysis compared DOAC users who also received an SSRI with DOAC users who received a non-SSRI antidepressant. That design keeps the comparison closer to patients who had an antidepressant indication.
- SSRI group: 35,782 people had DOAC+SSRI exposure in the cohort analysis.
- Comparison group: 39,745 people had DOAC+non-SSRI antidepressant exposure.
- Median age: DOAC+SSRI users were slightly younger, 73.1 years versus 75.4 years in the non-SSRI comparison group.
- Clinical mix: About 61% of both groups had atrial fibrillation, and about 30% had venous thromboembolism.
Researchers used propensity-score weighting, a statistical method that tries to balance measured differences between groups. It cannot remove every source of bias, but it reduces the chance that obvious baseline differences explain the result.
Major Bleeding Outcomes Did Not Rise in the Cohort Analysis
The headline cohort finding was a set of near-null estimates. After weighting, DOAC+SSRI use was not clearly associated with higher intracranial bleeding, gastrointestinal bleeding, or other bleeding than DOAC+non-SSRI antidepressant use.
- Intracranial bleeding: HR 1.16, with a 99% confidence interval from 0.62 to 2.20.
- Gastrointestinal bleeding: HR 1.09, with a 99% confidence interval from 0.83 to 1.41.
- Other bleeding: HR 1.01, with a 99% confidence interval from 0.78 to 1.29.
Those numbers do not prove the two-drug combination is risk-free. They mean this study did not find evidence that the SSRI group had higher bleeding risk than the non-SSRI antidepressant group for those outcomes in the cohort design.
Starting an SSRI During DOAC Use Showed a Smaller Safety Signal
The second design tested timing. In a case-crossover analysis, researchers looked only at people who had bleeding outcomes and compared each person with themselves across different time windows.
This self-controlled method can reduce confounding from stable patient traits, such as sex, long-term illness burden, or baseline frailty. It is especially useful for asking whether a recent medication change happened shortly before an event.
For intracranial and gastrointestinal bleeding, the case-crossover results did not show the same drug-interaction pattern.
The notable estimate was for other bleeding: starting an SSRI while already taking a DOAC had an odds ratio of 1.64, compared with OR 1.06 for SSRI monotherapy. The Wald test supported a difference between those estimates.
- Initiation of SSRI while taking DOAC: other bleeding OR 1.64, 99% CI 1.14 to 2.35.
- SSRI initiation without DOAC: other bleeding OR 1.06, 99% CI 1.01 to 1.11.
- Non-SSRI control: researchers did not find the same stronger interaction pattern when non-SSRI antidepressants were initiated in DOAC users.
Monitoring Matters Most When an SSRI Is Newly Started
These findings do not support avoiding SSRIs in every person taking a DOAC. Depression, anxiety, atrial fibrillation, venous thromboembolism, and stroke aftercare often overlap, and undertreating mental health symptoms can carry its own risks.
The first period after an SSRI is started may deserve extra attention in patients already using anticoagulation.
That attention could include reviewing other bleeding-risk drugs, checking kidney function, clarifying warning signs, and making sure the DOAC dose matches the indication and patient profile.
- Medication review: aspirin, antiplatelet drugs, nonsteroidal anti-inflammatory drugs, and other interacting medicines can change the bleeding-risk picture.
- Outcome specificity: the strongest finding was not for intracranial or gastrointestinal bleeding in the primary analyses.
- Timing: the case-crossover estimate focused on medication initiation, not stable long-term combined use.
- Comparison choice: the main cohort comparator was non-SSRI antidepressant use, not no antidepressant use.
Observational Data Leave Room for Residual Confounding
This was a large real-world study, but it was still observational. Prescribing decisions, bleeding history, frailty, alcohol use, over-the-counter drug use, and reasons for changing antidepressants may not be fully captured in routine records.
The source PDF was an author-accepted manuscript, meaning the study had been accepted but not yet passed through final publication formatting and correction at the time of the PDF.
The DOI should be checked for the version of record before final WordPress upload if the route is available.
Clinical takeaway: DOAC+SSRI use did not show a clear cohort-level increase in the major bleeding outcomes studied, but SSRI initiation during DOAC treatment remains a reasonable moment for closer medication-safety review.
Citation: DOI: 10.3399/BJGPO.2025.0267. Chau et al. Potential interactions between SSRIs and DOACs: population-based cohort and case-crossover study. BJGP Open. 2026.
Study Design: Population-based cohort plus modified case-crossover analysis using UK routine primary-care and linked health records.
Sample Size: 35,782 DOAC+SSRI users and 39,745 DOAC+non-SSRI antidepressant users in the cohort analysis.
Key Statistic: Cohort hazard ratios were near 1 for intracranial bleeding, gastrointestinal bleeding, and other bleeding; the case-crossover other-bleeding estimate was OR 1.64 for SSRI initiation while taking a DOAC.
Caveat: Observational prescribing and bleeding records can leave residual confounding, and live DOI/version-of-record checks are still pending because WordPress/REST DNS was unavailable in this run.





