TL;DR: A 2026 study in Translational Psychiatry found that three different plasma p-tau217 assays separated Alzheimer’s dementia from controls and frontotemporal degeneration with excellent accuracy, shifting the test from whether the marker works to which platform clinics can deploy.
Key Findings
- Three p-tau217 assays all performed strongly: The cohort included 39 cognitively unimpaired controls, 28 mild cognitive impairment (MCI) due to Alzheimer’s disease, 57 Alzheimer’s dementia cases, 70 subcortical ischemic vascular dementia cases, and 39 frontotemporal lobar degeneration cases.
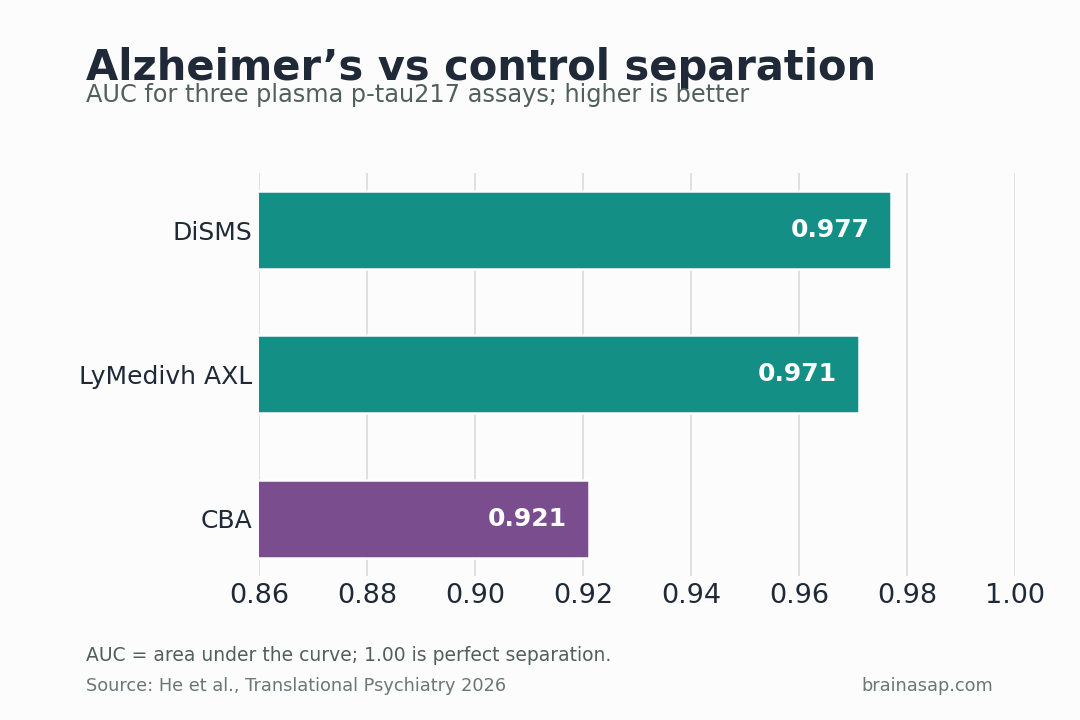
- All 3 novel assays cleanly separated Alzheimer’s dementia from controls: AUCs for Alzheimer’s dementia versus cognitively unimpaired controls were 0.977 for DiSMS, 0.971 for LyMedivh AXL, and 0.921 for CBA.
- Frontotemporal dementia separation was just as strong: The same assays reached AUCs of 0.973, 0.947, and 0.909 when distinguishing Alzheimer’s dementia from FTLD.
- Two platforms also picked up prodromal disease: DiSMS and LyMedivh AXL detected elevated p-tau217 in MCI due to Alzheimer’s disease and posted AUCs of 0.941 and 0.957 versus controls, while CBA trailed at 0.807.
- Specificity hit 100% across the board at optimal cutoffs: DiSMS and LyMedivh AXL matched the reference ALZpath Simoa assay with 94.4% sensitivity and 96.1% accuracy, while CBA delivered 88.9% sensitivity and 92.2% accuracy.
Source: Translational Psychiatry (2026) | He et al.
Blood-based Alzheimer’s biomarkers have felt fragile for years because so much of the evidence has come from one favored assay platform at a time.
This study is helpful because it asks a tougher test: if you change the chemistry and hardware, does p-tau217 still hold up?
Three p-tau217 Assays Tested Whether the Blood readout Generalizes
Alzheimer’s diagnosis has been moving steadily out of the “wait for memory collapse” era and into the biomarker era.
Three details anchor the result:
- Three p-tau217 assays all performed strongly: The cohort included 39 cognitively unimpaired controls, 28 mild cognitive impairment (MCI) due to Alzheimer’s disease, 57 Alzheimer’s dementia cases, 70 subcortical ischemic vascular dementia cases, and 39 frontotemporal lobar degeneration cases
- All 3 novel assays cleanly separated Alzheimer’s dementia from controls: AUCs for Alzheimer’s dementia versus cognitively unimpaired controls were 0.977 for DiSMS, 0.971 for LyMedivh AXL, and 0.921 for CBA
- Frontotemporal dementia separation was just as strong: The same assays reached AUCs of 0.973, 0.947, and 0.909 when distinguishing Alzheimer’s dementia from FTLD
The big attraction of plasma p-tau217 is that it promises something clinics need: a blood test that behaves like the disease, not just a rough risk marker.
But biomarker excitement tends to outrun replication.
One assay works well in one study, another company launches a different platform, and the field has to ask whether the readout belongs to the molecule or to the machine.
That is exactly what makes this study more helpful than a simple “new test looks promising” report.
Researchers compared three novel p-tau217 assays in the same real-world cohort, then checked how closely they matched the better-known ALZpath Simoa reference assay.
If p-tau217 is truly becoming clinic-ready, it should keep working even when the underlying lab technology changes.
What a 233-Person Chinese Cohort Could Test That Smaller Studies Could Not
The study recruited 233 participants from a longitudinal cohort at Tianjin Medical University General Hospital.
Crucially, the comparison was not just Alzheimer’s versus healthy aging.
The investigators also included people with mild cognitive impairment due to Alzheimer’s disease, subcortical ischemic vascular dementia, and frontotemporal lobar degeneration.
The reason is the hard clinical problem is rarely “Is this person normal or demented?” It is “What kind of neurodegeneration is this?” Biomarkers that only separate advanced Alzheimer’s from healthy controls are helpful, but they are not yet solving the everyday differential diagnosis problem.
The three assays represented three different technical approaches: a single-molecule method called DiSMS, a digital ELISA platform called LyMedivh AXL, and a flow-cytometry-based assay called CBA.
The reference comparison came from ALZpath Simoa, one of the most established p-tau217 platforms in the field.
The Best Number in the Paper Is Not 0.977 but the Cluster of Results Around It
The flashiest AUC in the study was 0.977, achieved by DiSMS for distinguishing Alzheimer’s dementia from cognitively unimpaired controls. The more important point was the cluster of results around it:
- Controls: AUCs were 0.977 for DiSMS, 0.971 for LyMedivh AXL, and 0.921 for CBA.
- FTLD: AUCs were 0.973, 0.947, and 0.909.
- Vascular dementia: performance dipped but remained helpful at 0.882, 0.834, and 0.829.
The real strength of the paper is that these values travel as a group.
Instead of one assay posting a great number while the others collapse, all three stayed in a reasonably strong range.
The central claim becomes more believable. The diagnostic readout appears to belong to p-tau217 itself, not only to one brand’s platform.
How Two Assays Reached 94.4% Sensitivity Without False Positives
Cutoff performance is where the paper becomes clinically informative rather than merely academic.
Using their optimal thresholds, the DiSMS and LyMedivh AXL assays both matched ALZpath Simoa with 94.4% sensitivity, 100% specificity, and 96.1% accuracy for distinguishing Alzheimer’s dementia from controls.
CBA did a bit worse, at 88.9% sensitivity and 92.2% accuracy, but it still kept specificity at 100%.
False positives are one of the biggest worries in early biomarker rollouts.
A test that labels non-Alzheimer’s patients as positive can create expensive downstream cascades of imaging, treatment evaluation, and fear.
The other encouraging detail is that the novel platforms tracked the reference assay reasonably well.
Correlations reached r = 0.890 for DiSMS and r = 0.737 for LyMedivh AXL, with CBA lower at 0.407 but still statistically significant.
- DiSMS: tracked ALZpath Simoa most closely, with r = 0.890.
- LyMedivh AXL: also aligned well, with r = 0.737.
- CBA: was weaker but still statistically significant, with r = 0.407.
In practical terms, the better two platforms were not just directionally similar to ALZpath Simoa. They were closely aligned.
Prodromal Alzheimer’s Is the More Important Battlefield
Late-stage Alzheimer’s is not where blood biomarkers will prove their real value.
The more important task is catching disease earlier, when patients still present as mild cognitive impairment and treatment decisions are less obvious.
That is where the paper’s platform differences start to matter.
DiSMS and LyMedivh AXL both detected elevated p-tau217 in MCI due to Alzheimer’s disease and produced AUCs of 0.941 and 0.957 against controls.
CBA, by contrast, dropped to 0.807. That is not failure, but it is enough of a gap to suggest that not every p-tau217 assay is equally good at the earliest stages.
Researchers also found no significant correlation between p-tau217 concentration and Mini-Mental State Examination scores in established Alzheimer’s disease.
That fits the current biomarker argument.
p-tau217 appears to be better as a pathology readout than as a coarse severity meter once dementia is already underway.
Blood p-tau217 Still Needs Cohort and Assay Validation
p-tau217 is no longer a one-platform result. Multiple assay designs identified Alzheimer’s disease and differentiated it from other dementias with strong performance, at least in this Chinese cohort.
That said, the paper is not the final word on rollout. Sample sizes were still modest, and different assays were run on somewhat different subsamples.
The cohort also did not use positron emission tomography (PET) imaging or cerebrospinal fluid biomarkers to exclude hidden Alzheimer’s pathology from every non-Alzheimer’s group.
PET uses radioactive tracers to map biology in living tissue, so it can help verify amyloid or tau pathology when blood results are uncertain.
The limitation matters most for the vascular dementia comparison, where mixed pathology can flatten the apparent separation.
Still, this is the sort of study the field needed.
It suggests clinics do not have to wait for one perfect monopoly assay before blood-based Alzheimer’s testing becomes practical.
The more realistic future is likely a handful of p-tau217 platforms that all work well enough, with the main test shifting to cost, access, and quality control rather than whether the biomarker itself is real.
Citation: DOI: 10.1038/s41398-026-04043-0. He et al. Diagnostic performance of plasma p-tau217 levels measured with different assays for Alzheimer’s disease. Translational Psychiatry. 2026.
Study Design: Cohort study
Sample/Model: 233 participants across 5 diagnostic groups: The cohort included 39 cognitively unimpaired controls, 28 MCI due to Alzheimer’s disease, 57 Alzheimer’s dementia cases, 70 subcortical ischemic vascular dementia cases, and 39 frontotemporal lobar degeneration cases.
Key Statistic: All 3 novel assays cleanly separated Alzheimer’s dementia from controls: AUCs for Alzheimer’s dementia versus cognitively unimpaired controls were 0.977 for DiSMS, 0.971 for LyMedivh AXL, and 0.921 for CBA.
Caveat: Single-study evidence; interpret with the source design and sample.