TL;DR: A 2026 population-based study in The Canadian Journal of Psychiatry found that early-life adversity scores were linked to higher group-level mental health risk but performed poorly for identifying which Canadian adults had anxiety, mood disorders, substance use disorders, or suicidality.
Key Findings
- 7,608 Canadian adults: Researchers analyzed nationally representative 2022 survey data collected during the COVID-19 pandemic.
- Six adversity items: Early-life adversity (ELA) covered direct violence or abuse before age 16, including physical abuse, sexual abuse, and exposure to domestic violence.
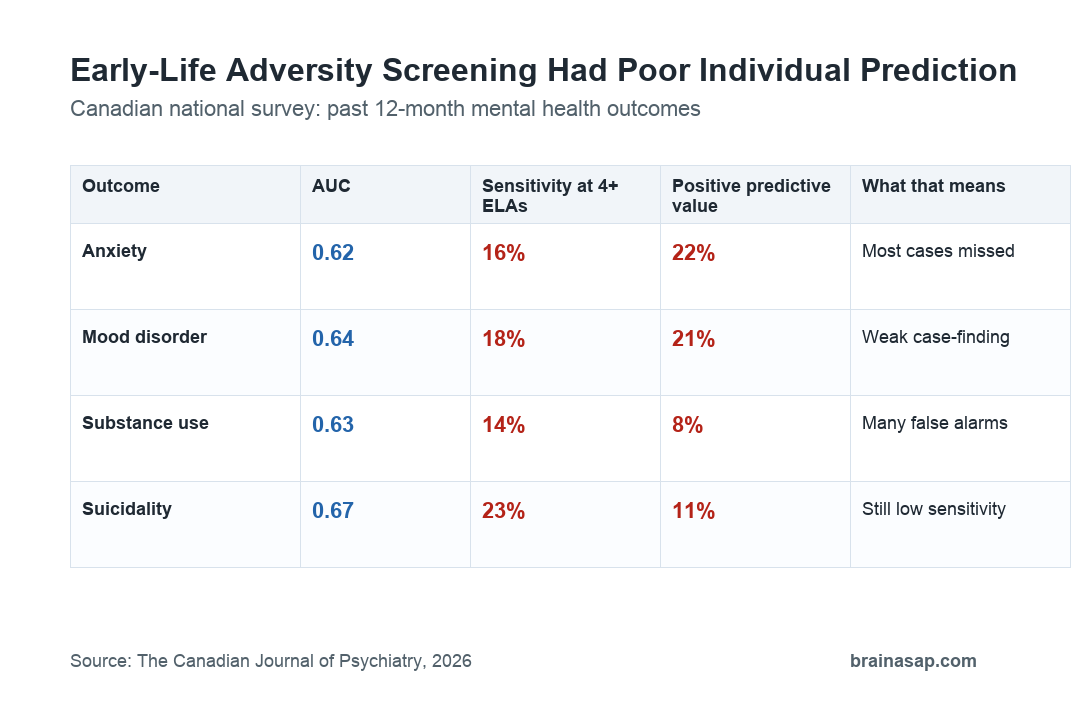
- Poor AUC values: ELA scores showed poor discrimination across mental health domains, with AUC values from 0.62 to 0.67.
- Low high-risk sensitivity: A 4-or-more ELA cut-off identified only 14% to 23% of people with the measured mental health outcomes.
- High specificity, low PPV: The same cut-off had high specificity of 0.93 to 0.94, but positive predictive values were only 0.08 to 0.22.
Source: The Canadian Journal of Psychiatry (2026) | Johnson et al.
Early-life adversity is clearly linked to mental health risk at the population level. The harder question is whether a short adversity score can decide which individual person needs intervention.
This study tested that screening question directly in Canada. ELA scores tracked group risk, but they were weak tools for individual case-finding.
Canadian Survey Data Tested Individual Risk Prediction
The sample came from the Mental Health and Access to Care Survey, a nationally representative Statistics Canada survey conducted from March to July 2022.
Researchers started with 9,409 adults, removed respondents with missing outcome or adversity data, and analyzed a final sample of 7,608 adults. The weighted sample was about 51% female, with a mean age near 48 years.
- Mental health outcomes: The survey assessed past-year mood disorders, anxiety disorders, substance use disorders, and suicidality.
- Diagnostic instrument: Outcomes came from the World Mental Health-Composite International Diagnostic Interview.
- Adversity score: ELA was counted from 0 to 6 based on direct violence, physical abuse, sexual abuse, and domestic-violence exposure before age 16.
The pandemic timing mattered because distress was elevated in many populations. If adversity screening worked better when mental health problems were more common, this sample gave it a reasonable chance to show that.
More Adversity Raised Group-Level Odds
At the group level, the expected relationship appeared. Adults reporting more ELAs had higher odds of mental health problems than adults reporting no ELA.
For people reporting 4 or more ELAs, odds were about fourfold higher for depression, anxiety, and substance use, and nearly eightfold higher for suicidality, compared with people reporting no ELA.
- Anxiety prevalence: Past-year anxiety disorders were the most common measured outcome at 9.81%.
- Mood prevalence: Mood disorders were present in 8.21% of the weighted sample.
- Suicidality prevalence: Suicidal thoughts, plans, or attempts were present in 3.58%.
Those findings support the public-health point: adversity burden is associated with mental health risk. They do not automatically support using an ELA score as a clinical allocation tool.
AUC Values Stayed in the Poor Prediction Range
AUC, or area under the curve, measures how well a score separates people with an outcome from people without it. Values around 0.5 are chance-level, while values above 0.8 are generally considered good discrimination.
ELA scores did not approach that range. AUC was 0.62 for anxiety, 0.64 for mood disorders, 0.63 for substance use disorders, and 0.67 for suicidality.
The study’s practical message was that population-level association did not translate into strong individual prediction. A randomly selected person with a mental health problem was only modestly more likely to have a higher ELA score than a randomly selected person without one.
The 4-ELA Cut-Off Missed Most Cases
The common high-risk threshold was 4 or more ELAs. That threshold had high specificity, meaning people below the cut-off were usually not classified as high risk.
But sensitivity was low. The threshold identified only 16% of anxiety cases, 18% of mood-disorder cases, 14% of substance-use cases, and 23% of suicidality cases.
- False negatives: Many people with mental health problems reported fewer than 4 ELAs and would not be flagged.
- False positives: Many people above the high-risk threshold did not have the measured mental health outcome.
- Low PPV: Positive predictive values ranged from 0.08 to 0.22, depending on the outcome.
That combination is difficult for intervention allocation. A screen can look useful in group graphs while still missing many individuals who need help.
ELA Scores Need Broader Clinical Context
The study does not argue that childhood adversity is unimportant. It argues that a simple count of direct or severe adversities is not enough to decide individual mental health risk.
Adversity scores also omit factors that can change risk direction, including timing, chronicity, social support, discrimination, emotional neglect, resilience, current stress, and access to care.
A better screen would need to combine adversity with current symptoms, protective relationships, functioning, and care access.
- Measurement limit: The study used retrospective reports, which can be affected by recall and current mental health.
- Scope limit: The adversity module focused on direct violence and abuse, not every form of childhood stress.
- Setting limit: Findings apply to universal screening in the Canadian adult population, not necessarily acute clinical settings with higher base rates.
The practical takeaway is straightforward: ELA screening may help describe population burden, but it should not be used by itself to assign individual mental health intervention.
Citation: DOI: 10.1177/07067437261442418. Johnson et al. Predicting Mental Health Risk from Early-Life Adversity: A Population-Based Study of Canadian Adults. The Canadian Journal of Psychiatry. 2026.
Study Design: Nationally representative cross-sectional survey analysis of Canadian adults.
Sample Size: 7,608 adults with complete mental health and early-life adversity data.
Key Statistic: ELA score AUC values were 0.62 to 0.67, and the 4-or-more cut-off had sensitivity of 0.14 to 0.23.
Caveat: The study used retrospective adversity reports and tested universal screening, not a full clinical risk model with protective factors.





