TL;DR: A 2026 randomized clinical trial in JAMA Network Open found that one supervised 30 mg/70 kg psilocybin dose plus cognitive behavioral therapy produced 40.5% six-month smoking abstinence versus 10.0% with a nicotine patch plus the same therapy.
Key Findings
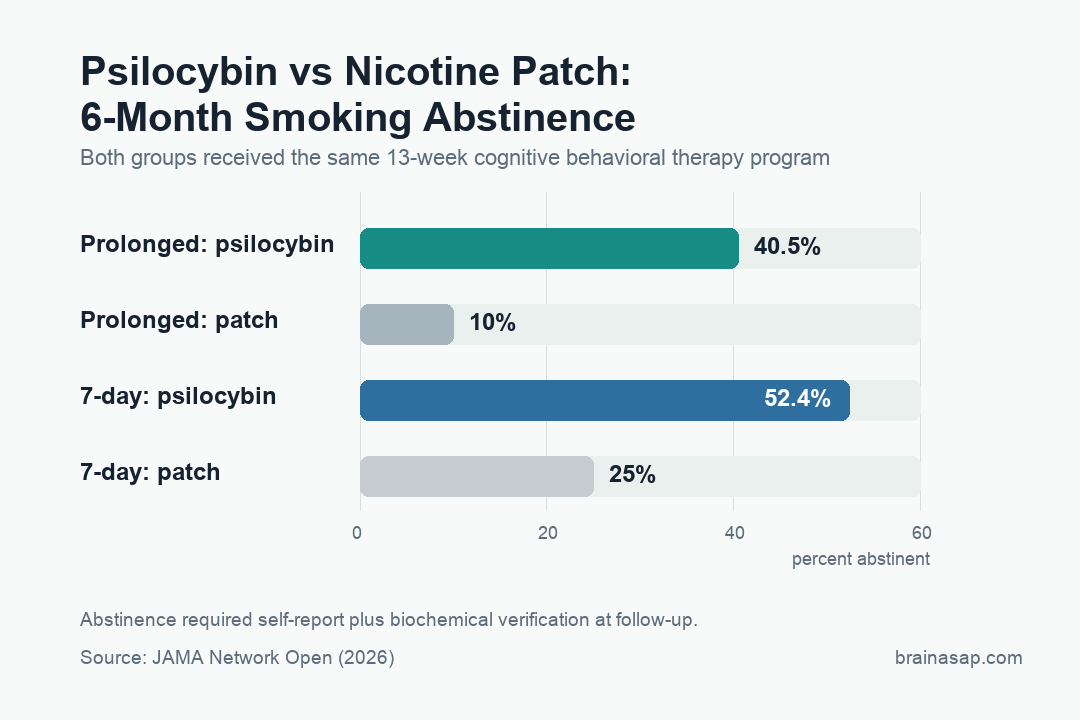
- 40.5% vs. 10% prolonged abstinence at 6 months: 17 of 42 psilocybin participants stayed biochemically verified smoke-free; only 4 of 40 patch participants did. Odds ratio 6.12 (95% CI 1.99-23.26, p=0.003).
- 52.4% vs. 25% 7-day point prevalence abstinence: Psilocybin doubled the standard secondary endpoint at 6 months (OR 3.30, 95% CI 1.32-8.70, p=0.01).
- One single high dose of psilocybin (30 mg/70 kg): Delivered on the target quit date, paired with the same 13-week cognitive behavioral therapy program both groups received.
- Average smoker had failed multiple prior quit attempts: 82 participants, mean age 47.6, 16 cigarettes per day, median 6 prior attempts to quit — not first-timers.
- Safety and smoking-volume signals were secondary: No serious adverse events were attributed to either drug, and participants who did not fully quit still smoked fewer cigarettes after psilocybin.
Source: JAMA Network Open (2026) | Johnson et al.
Tobacco kills about 8 million people a year worldwide, and standard quit aids such as nicotine patches, gum, and prescription medications produce real but modest gains.
Most smokers who try to quit relapse, often multiple times.
A randomized trial at Johns Hopkins compared the nicotine patch with psilocybin-assisted therapy, and the psilocybin arm produced a much higher 6-month abstinence rate.
The Trial Design That Made the Comparison Fair
Psychedelic addiction studies have an obvious credibility risk because patients know they are getting a powerful drug, and expectancy can drive results.
The Johns Hopkins team handled this by making the comparison group an active treatment, not a placebo. Both arms got the same 13-week manualized cognitive behavioral therapy designed for smoking cessation.
Both groups had four preparatory counseling sessions before the target quit date and met with facilitators afterward to integrate insights into ongoing quit support.
The only difference was what happened on quit day.
The psilocybin group received a single 30 mg/70 kg dose under standard psychedelic-therapy conditions: lying on a couch, eye shades, curated music, and two trained facilitators monitoring throughout.
The nicotine patch group started an 8-10 week regimen of FDA-approved patches dosed by their typical cigarette consumption.
How the Trial Verified Quit Status — Beyond Self-Report
Smoking-cessation trials are notorious for self-report problems. The Johns Hopkins design built in biochemical verification at every follow-up:
- Exhaled carbon monoxide: Captures smoking in the prior 24 hours.
- Urine cotinine: Detects nicotine metabolites from the prior week.
- Self-report combined with both biochemical markers: A participant counted as abstinent only if all three measures agreed.
Triple verification reduces the most common reason psychedelic addiction studies can look stronger than they are: patients telling researchers what they want to hear.
The 40.5% prolonged abstinence figure is biochemically verified, not self-reported.
Psilocybin Produced Six Times the Odds of 6-Month Abstinence
An OR of 6.12 means psilocybin participants had over six times the odds of staying quit compared with patch users at 6 months.
In addiction medicine, that is a different magnitude than typical incremental treatment improvements:
- Standard nicotine replacement vs. placebo: Roughly doubles quit rates (OR ~2).
- Varenicline (Chantix) vs. placebo: About 2-3x quit rates.
- Bupropion vs. placebo: About 1.6x quit rates.
- Psilocybin vs. nicotine patch (this trial): 6.12x quit rates.
The catch is that psilocybin was not being compared to placebo. It was being compared to one of the established active treatments, which makes the effect size more striking.
Why This Isn’t the Final Word — Yet
The Johns Hopkins team is appropriately careful about what their trial does and does not show.
The pilot is unblinded: participants and investigators knew which treatment was being delivered, which can amplify expectancy effects in both directions. The sample is 82 people.
The trial was not designed to identify which patients respond best to psilocybin or which mechanisms drive the effect.
What it does show: a single dose of psilocybin, delivered with structured psychological support, produced smoking cessation rates that exceeded a first-line standard treatment in psychiatrically healthy smokers.
The result supports a phase 3 trial and further review of scheduling decisions that make psilocybin research difficult.
The Mechanism Isn’t About Nicotine Receptors
Most cessation aids work by manipulating nicotine biology directly: replacing it with patches or gum, partially blocking it with varenicline, or dampening reward with bupropion.
Psilocybin does not work through nicotine receptors. It binds serotonin receptors and produces a temporary altered state of consciousness.
The therapeutic effect appears to come from psychological flexibility: a temporarily loosened relationship with habitual self-narratives, including the narrative that a person is a smoker.
If that mechanism holds up, the implications extend beyond tobacco.
Alcohol use disorder, opioid dependence, and other substance use conditions share the same problem: entrenched habit patterns that people cannot talk themselves out of.
The Johnson trial did not test those applications, but the broader addiction-treatment question now has stronger funding rationale.
What This Means Now and What Still Has to Happen
Nothing in this trial means smokers should be seeking out psilocybin outside clinical research.
The drug remains Schedule I, and the trial used screened, psychiatrically healthy adults under medical supervision with two trained facilitators per session.
Recreational psilocybin use carries different risks in different contexts.
For the science, a single supervised psychedelic dose produced quit rates that more than doubled the best-established active treatment.
The result should accelerate phase 3 testing, expand mechanistic research into psychedelic-assisted addiction therapy, and force regulators to consider whether current scheduling reflects 2026 evidence or 1970s politics.
Citation: DOI: 10.1001/jamanetworkopen.2026.0972. Johnson et al. Psilocybin or Nicotine Patch for Smoking Cessation: A Pilot Randomized Clinical Trial. JAMA Network Open. 2026.
Study Design: Pilot randomized clinical trial at Johns Hopkins Bayview Medical Center; participants and investigators unblinded with optional crossover after primary endpoint; both arms received 13-week manualized cognitive behavioral therapy.
Sample Size: 82 psychiatrically healthy adult smokers (mean age 47.6, 49 male, ~16 cigarettes/day, median 6 prior quit attempts); 68 (82.9%) completed the 6-month follow-up. 42 randomized to psilocybin, 40 to nicotine patch.
Key Statistic: 6-month prolonged biochemically verified abstinence: 40.5% (psilocybin) vs. 10% (patch); OR 6.12 (95% CI 1.99-23.26, p=0.003). 7-day point prevalence abstinence: 52.4% vs. 25%; OR 3.30 (95% CI 1.32-8.70, p=0.01). Psilocybin group smoked ~half as many daily cigarettes after target quit date.
Caveat: Pilot trial, unblinded, 82 participants; psychiatrically healthy adults with cardiovascular screening; not a phase 3 result; mechanism (psychological flexibility vs. neurobiological) not directly tested.