TL;DR: A 2026 medRxiv preprint applied the AT(N) framework, an Alzheimer’s disease biomarker system for amyloid, tau, and neurodegeneration, to 84 older adults with focal epilepsy and found that only 32.1% had normal blood biomarkers, while early-onset epilepsy carried higher odds of biomarker abnormality.
Key Findings
- Epilepsy cohort: Researchers analyzed focal epilepsy participants from the Brain Aging and Cognition in Epilepsy study, with mean age 66.3 years.
- AT(N) blood biomarkers: The amyloid/tau/neurodegeneration framework used plasma Aβ42/Aβ40 for amyloid, p-tau181 for tau, and neurofilament light chain (NfL), a neuronal-injury protein, for neurodegeneration.
- 32.1% normal profiles: Blood-based classification put 27 participants in the normal group, 31 in the Alzheimer’s disease continuum, and 26 in non-AD pathologic change.
- Early-onset epilepsy carried higher odds: Early-onset epilepsy was linked to higher odds of any biomarker abnormality than late-onset unexplained epilepsy, with adjusted odds ratio 8.84.
- Blood markers did different jobs: Higher p-tau181, a phosphorylated tau blood marker, was independently associated with lower word-list delayed recall, while replacing NfL with hippocampal volume shifted AT(N) classification.
Source: medRxiv preprint (2026) | Arrotta et al.
Epilepsy creates a hard interpretation problem for Alzheimer’s blood tests. Seizures, seizure duration, medication burden, and focal brain injury can all shape cognition and neuronal-injury markers, so an Alzheimer’s biomarker framework needs epilepsy-specific calibration.
Older Adults With Epilepsy Have Elevated Dementia Risk
Older adults with epilepsy have an estimated 2- to 4-fold higher risk of dementia than the general population. Alzheimer’s disease and epilepsy also overlap biologically: seizures can appear in Alzheimer’s disease, and epileptic activity can interact with amyloid and tau pathways.
The complication is that epilepsy is not Alzheimer’s disease by another name. Cognition in epilepsy can be shaped by seizure history, anti-seizure medication burden, seizure focus, sleep disruption, vascular risk, and structural brain injury.
The blood-biomarker framework is attractive but tricky in this setting:
- Amyloid marker: Plasma Aβ42/Aβ40 was used as the amyloid component, with a lower ratio indicating greater amyloid burden.
- Tau marker: Plasma p-tau181 was used as the tau component, while p-tau217 was examined continuously because it can be sensitive to amyloid-linked pathology.
- Neurodegeneration marker: NfL was used for neurodegeneration, but NfL can rise after neuronal injury and is not specific to Alzheimer’s disease.
- Epilepsy-specific alternative: Researchers also tested hippocampal volume, a structural MRI measure, as another way to define neurodegeneration.
The preprint status is a major context point. These findings have not been peer reviewed and should not guide clinical decisions by themselves.
BrACE Study Included 84 Focal Epilepsy Participants
The sample came from the Brain Aging and Cognition in Epilepsy, or BrACE, study. BrACE is a multicenter study of adults aged 55 years or older with early-onset epilepsy or late-onset unexplained epilepsy.
After excluding 9 people with missing AT(N) data, the biomarker analysis included 84 participants. Mean age was 66.3 years, 57.1% were female, and the cohort was mostly White.
The epilepsy profile was clinically substantial:
- Median duration: Median epilepsy duration was 20 years, with a wide interquartile range of 5 to 37.5 years.
- Temporal lobe epilepsy: 48.8% had temporal lobe epilepsy, and left-sided seizure onset was the most common side.
- Drug resistance: 61.9% met criteria for drug-resistant epilepsy.
- Recent seizure timing: Only 3 participants had a seizure within 24 hours of blood draw, reducing but not removing concern about acute seizure-related biomarker effects.
Cognition was assessed with the International Classification of Cognitive Disorders in Epilepsy, or IC-CoDE, and the Montreal Cognitive Assessment (MoCA), a cognitive screening test. Memory was also tested with word-list delayed recall.
Blood AT(N) Profiles Were Often Abnormal in Epilepsy
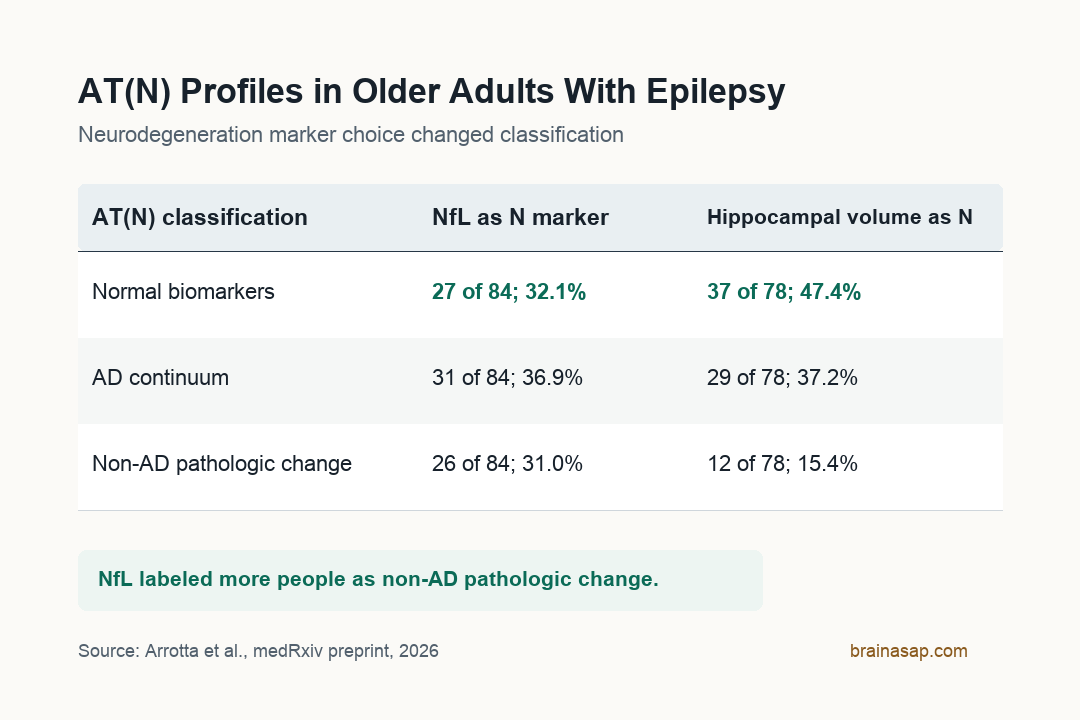
The blood-based AT(N) classification placed 32.1% of participants in the normal biomarker group. Another 36.9% were classified in the Alzheimer’s disease continuum, and 31.0% showed non-AD pathologic change.
The normal group was younger and had shorter epilepsy duration. Longer epilepsy duration was associated with higher NfL levels, with a per-10-year beta estimate of 5.72 and p = 0.013.
APOE-ε4 carriers were enriched in the Alzheimer’s disease continuum group. APOE-ε4 is a genetic risk variant linked to higher Alzheimer’s disease risk, so that enrichment supports the idea that at least part of the biomarker classification captured Alzheimer’s-related biology rather than random epilepsy noise.
When researchers compared early-onset epilepsy with late-onset unexplained epilepsy, categorical AT(N) profile groups did not differ significantly at first. But after collapsing the profiles into normal versus abnormal blood biomarkers, early-onset epilepsy had adjusted odds ratio 8.84 for biomarker abnormality compared with late-onset unexplained epilepsy.
Individual biomarker analyses pointed toward several drivers in the early-onset group:
- Higher p-tau217: Early-onset epilepsy was associated with higher p-tau217, with beta 1.30 and p = 0.010.
- Higher NfL: Early-onset epilepsy was associated with higher NfL, with beta 29.65 and p = 0.003.
- Greater amyloid burden: Early-onset epilepsy had a lower Aβ42/Aβ40 ratio, consistent with greater amyloid burden, with p = 0.048.
- No p-tau181 onset difference: p-tau181 did not significantly differ between early-onset and late-onset unexplained epilepsy groups.
p-tau181 Was Linked to Word-List Memory, Not MoCA
The cognitive result was not a simple “abnormal profile equals worse cognition” finding. Categorical AT(N) groups were not significantly associated with IC-CoDE cognitive phenotype or MoCA total score.
The null cognitive result is clinically relevant because epilepsy-related cognition has many causes. A person can have abnormal amyloid, tau, or NfL and still have cognitive symptoms shaped mainly by seizures, medications, focal brain networks, mood, sleep, or vascular disease.
The more specific memory finding came from continuous biomarker analysis. Higher log-transformed p-tau181 was associated with lower word-list delayed recall after covariate adjustment, with beta -5.59, 95% confidence interval -10.31 to -0.86, and p = 0.021.
Removing one p-tau181 outlier produced a similar but stronger association. In that sensitivity analysis, beta was -7.58, with 95% confidence interval -13.77 to -1.39 and p = 0.017.
The separation between p-tau217 and p-tau181 is one of the more useful biological details:
- p-tau217 and amyloid: p-tau217 and Aβ42/Aβ40 helped distinguish early-onset from late-onset unexplained epilepsy.
- p-tau181 and memory: p-tau181 was the marker tied to word-list delayed recall.
- Possible interpretation: p-tau217 can reflect upstream amyloid-linked biology, while p-tau181 can sit closer to memory-relevant tau processes in this epilepsy cohort.
NfL and Hippocampal Volume Changed the Neurodegeneration Picture
The neurodegeneration marker changed the classification. With NfL as the N marker, 32.1% were normal and 31.0% had non-AD pathologic change. With hippocampal volume substituted for NfL, 47.4% were normal and 15.4% had non-AD pathologic change.
NfL and total hippocampal volume were not significantly correlated, with Spearman’s r = -0.155 and p = 0.174. That means the two markers were not interchangeable in this cohort.
For epilepsy, the distinction is practical.
NfL can capture broad neuronal injury, including injury related to seizure burden or chronic epilepsy duration. Hippocampal volume can better capture structural atrophy, but it can miss diffuse neurodegeneration or be complicated by epilepsy-related hippocampal change.
The preprint therefore supports multimodal interpretation rather than a single blood-test answer. A biomarker panel designed for typical Alzheimer’s disease aging may need epilepsy-specific calibration before it can be used for risk stratification.
Preprint Limits Keep This in the Risk-Research Lane
The paper is useful because it tests a modern Alzheimer’s biomarker framework in a group often excluded from Alzheimer’s trials. The result also gives future studies several measurable targets: AT(N) class, p-tau181, p-tau217, NfL, hippocampal volume, seizure duration, and memory change.
Several limits keep the interpretation cautious:
- Preprint status: The report has not been peer reviewed, and the medRxiv page states that it should not guide clinical practice.
- Modest sample: The 84-person sample forced researchers to collapse 8 possible AT(N) combinations into 3 broader groups.
- Mostly cognitively intact cohort: Limited cognitive impairment may have reduced the ability to detect biomarker-cognition relationships.
- Plasma threshold uncertainty: Blood biomarker cutpoints validated in typical aging populations do not translate cleanly to epilepsy.
- NfL specificity problem: NfL can reflect seizure-related neuronal injury, not only neurodegeneration in the Alzheimer’s disease sense.
The most defensible conclusion is that Alzheimer’s-related blood biomarkers can help characterize neurodegenerative risk in older adults with epilepsy, but the framework needs epilepsy-adapted validation.
Longitudinal BrACE data should be more informative than this cross-sectional snapshot. The key questions are whether AT(N) profiles predict cognitive decline over time, whether seizure activity changes biomarker trajectories, and whether epilepsy patients need different biomarker thresholds before blood tests can inform clinical monitoring.
Citation: DOI: 10.64898/2026.04.24.26351489. Arrotta et al. AT(N) Framework in Older Adults with Epilepsy: Plasma Biomarkers and Associations with Demographic, Clinical, and Cognitive Features. medRxiv. 2026.
Study Design: Cross-sectional plasma biomarker and cognition analysis from the multicenter BrACE cohort; preprint, not peer reviewed.
Sample Size: 84 adults aged 55 years or older with focal epilepsy and complete AT(N) biomarker data.
Key Statistic: Only 32.1% had normal blood-based AT(N) profiles; early-onset epilepsy was linked to higher odds of biomarker abnormality, adjusted odds ratio 8.84.
Caveat: Preprint status, modest sample size, mostly cognitively intact cohort, and plasma biomarker thresholds that may not translate cleanly to epilepsy.