TL;DR: A 2026 meta-analysis in Sleep and Breathing found that GLP-1 drugs, metabolic hormone medications involved in glucose, appetite, and weight regulation, were linked to fewer obstructive sleep apnea breathing events in adults with obesity.
Key Findings
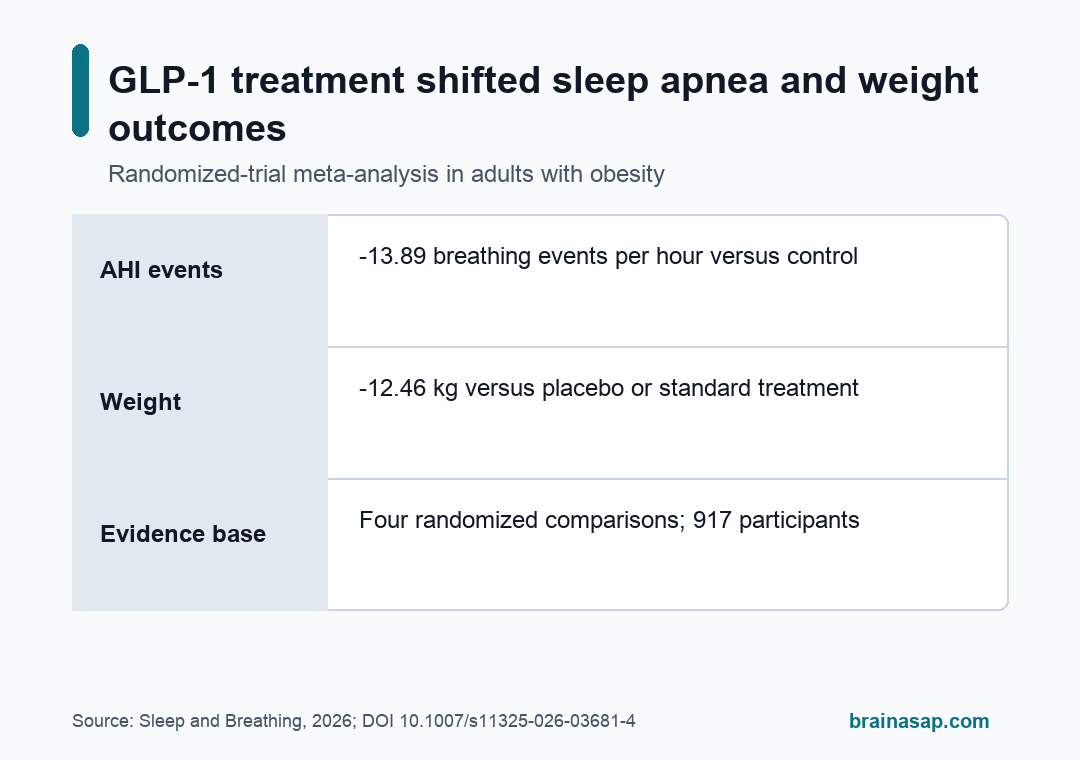
- Sleep apnea events fell: GLP-1 treatment reduced apnea-hypopnea index (AHI), a count of breathing interruptions per hour of sleep, by 13.89 events per hour versus control.
- Weight also changed: The pooled GLP-1 groups lost 12.46 kg more than placebo or standard-treatment groups.
- Blood pressure moved modestly: Systolic blood pressure was 4.86 mmHg lower, and diastolic blood pressure was 1.45 mmHg lower.
- Tirzepatide drove the largest sleep signal: The subgroup estimate was -23.80 AHI events per hour for tirzepatide versus -5.20 for liraglutide.
- The evidence was still narrow: Only four randomized trial comparisons with 917 participants were included, and treatment regimens differed across trials.
Source: Dandamudi et al. Sleep and Breathing. 2026.
Obstructive sleep apnea (OSA) happens when the upper airway repeatedly narrows or closes during sleep. OSA can mean repeated oxygen drops, sleep fragmentation, daytime sleepiness, and added cardiometabolic strain.
The new analysis looked at whether GLP-1 receptor agonists can change measured breathing-event burden in adults whose OSA is tied partly to obesity.
These medications include liraglutide and tirzepatide. They reduce appetite and support weight loss through brain and gut hormone pathways, which makes them relevant to OSA when excess weight is one driver of airway collapse.
Four Randomized Trial Comparisons Tested GLP-1 Drugs in OSA
The meta-analysis pooled four randomized controlled trial comparisons involving 917 adults. Across those trials, 458 participants received a GLP-1 based therapy and 459 participants received placebo or standard treatment.
The trials were not identical. OSA can be driven by weight, airway anatomy, muscle tone, ventilatory control, or a mix of factors.
The meta-analysis therefore gives a class-level estimate, not a guarantee that every patient with OSA will respond in the same way.
- Liraglutide trial without CPAP: One study tested liraglutide 3.0 mg in adults with obesity and moderate-to-severe OSA who could not or would not use continuous positive airway pressure (CPAP).
- Liraglutide plus CPAP: Another study tested liraglutide in people with type 2 diabetes and severe OSA while participants were using CPAP.
- Tirzepatide trials: Two trial comparisons tested tirzepatide in adults with obesity and moderate-to-severe OSA, with different background positive-airway-pressure contexts.
The design mix reflects real clinical variation. It also makes the pooled estimate more cautious than a single clean drug-versus-placebo trial.
AHI Improved by About 14 Fewer Breathing Events Per Hour
The primary sleep outcome was apnea-hypopnea index (AHI). AHI counts apneas and hypopneas per hour of sleep, so a lower value means fewer measured breathing interruptions.
Compared with controls, GLP-1 treatment was associated with an average 13.89-event-per-hour reduction in AHI. The 95% confidence interval ran from -22.86 to -4.92 events per hour.
That is a clinically meaningful direction for moderate-to-severe OSA. In the paper’s framing, a person with 30 or more AHI events per hour is in the severe range, while 15 to 29.9 events per hour is moderate OSA.
A reduction of this size can shift some patients toward a less severe category, although the paper did not mean that medication alone eliminated OSA for everyone.
- AHI outcome: GLP-1 therapy was linked to -13.89 events per hour versus control.
- Weight outcome: Body weight was -12.46 kg versus control.
- Systolic pressure: Systolic blood pressure was -4.86 mmHg.
- Diastolic pressure: Diastolic blood pressure was -1.45 mmHg.
The AHI estimate had high statistical heterogeneity, meaning the trial estimates varied more than would be expected from chance alone. That is one reason the pooled number should be read as a strong signal with important context, not as a single uniform treatment effect.
Tirzepatide Had a 23.80-Event AHI Estimate Versus 5.20 for Liraglutide
The subgroup analysis separated liraglutide from tirzepatide. Liraglutide was associated with a 5.20-event-per-hour AHI reduction, while tirzepatide was associated with a 23.80-event-per-hour AHI reduction.
Tirzepatide is not a pure GLP-1 drug. It also activates glucose-dependent insulinotropic polypeptide (GIP) pathways, so the paper treated it as a dual GIP/GLP-1 receptor agonist.
The larger AHI estimate may reflect stronger weight loss, different metabolic effects, trial design, follow-up duration, or all of those factors together.
The subgroup difference for AHI was statistically significant. Blood pressure differences between the two drug classes were less clear, even though both moved systolic blood pressure in the favorable direction.
- Drug class matters: Tirzepatide had the larger AHI estimate in this analysis.
- Weight loss may be central: Larger weight changes can reduce mechanical load on the upper airway.
- OSA is not only weight: Airway anatomy, neuromuscular control, and ventilatory drive can still limit response.
CPAP Context Changed How the Evidence Should Be Read
CPAP keeps the airway open mechanically during sleep. GLP-1 based medications act through weight and metabolic pathways.
Those are different treatment routes, so the paper did not frame GLP-1 therapy as a simple replacement for CPAP.
The evidence is strongest for a narrower interpretation: in adults with obesity and OSA, especially when cardiometabolic risk is part of the clinical picture, GLP-1 based treatment may reduce sleep-disordered breathing while also improving body weight and blood pressure.
The included studies handled CPAP differently. One liraglutide trial excluded people who could use CPAP, while another required CPAP.
The tirzepatide publication included separate trial contexts. That variation is clinically useful, but it also means the pooled estimate should not be used to decide whether an individual patient can stop airway therapy.
- Mechanical treatment: CPAP directly splints the airway open during sleep.
- Metabolic treatment: GLP-1 and GIP/GLP-1 drugs can reduce weight and metabolic stressors that worsen OSA.
- Combined care: Some patients may need airway therapy, weight-focused treatment, positional therapy, oral appliances, or surgery depending on the dominant OSA mechanism.
Semaglutide Was Not Tested in These OSA RCTs
A practical caveat is that semaglutide, one of the most familiar GLP-1 medications, was not directly tested in the randomized OSA trials included in this review. The paper discussed liraglutide and tirzepatide evidence, not a semaglutide-specific OSA estimate.
The trial base was also small for a treatment question with major public interest. The included comparisons differed in drug, dose, follow-up time, CPAP background, and metabolic profile.
One study included people with type 2 diabetes. Others were centered on obesity and moderate-to-severe OSA.
Main limitation: the average estimate does not identify which patients respond because weight loss is the main driver, which respond because of broader metabolic changes, and which have OSA mechanisms that would remain despite medication.
In practice, GLP-1 based therapy reduced AHI in randomized evidence, with the largest estimate for tirzepatide.
The finding supports these medications as part of OSA management in selected patients with obesity, while leaving CPAP and other airway-directed care on the table.
Citation: DOI: 10.1007/s11325-026-03681-4. Dandamudi et al. Efficacy of GLP-1 Receptor agonists in treating Obstructive sleep apnea: A systematic review and meta-analysis of cardiometabolic and respiratory outcomes. Sleep and Breathing. 2026;30:138.
Study Design: Systematic review and meta-analysis of randomized controlled trial comparisons.
Sample Size: Four randomized trial comparisons with 917 adults, including 458 in GLP-1 based treatment groups and 459 in control groups.
Key Statistic: GLP-1 based therapy reduced AHI by 13.89 events per hour versus control; tirzepatide subgroup estimate was -23.80 events per hour.
Caveat: Trial regimens, CPAP background, diabetes status, follow-up duration, and drug class differed across the small evidence base.





