TL;DR: A 2026 analysis in Journal of Korean Medical Science identified PIK3CG, PRKCD, and TRIM22 as glioblastoma gene markers linked to worse survival and stronger immune-activity signals in IDH-wildtype tumors.
Key Findings
- 12,041-gene screen: Researchers screened tumor expression data to find genes tied to both poor prognosis and immune activation in grade IV glioma.
- 775 tumor cases: The analysis used TCGA data from 525 cases and CGGA validation data from 250 cases, plus 1,152 GTEx normal brain samples.
- 372 IDH-wildtype cases: The survival validation focused on the modern glioblastoma definition by excluding IDH-mutant and unknown-IDH cases where possible.
- Three marker genes: High PIK3CG, PRKCD, and TRIM22 expression remained associated with poorer overall survival after adjustment.
- Machine-learning signal: A survival model reached a 60-month AUC of 0.787, and a gradient-boosting model reported RMSE 0.059 with R2 0.996.
Source: Journal of Korean Medical Science (2026) | Han et al.
Glioblastoma (GBM) is the most aggressive primary malignant brain tumor. Even with surgery, radiation, and temozolomide chemotherapy, median survival is often reported around 14 to 16 months.
The Han analysis asked why immune activity in GBM does not always mean better survival. It looked for genes that rose with immune markers but still tracked worse outcomes.
PIK3CG PRKCD and TRIM22 Emerged From a Survival-Immune Screen
The workflow began with 12,041 candidate genes in The Cancer Genome Atlas grade IV glioma dataset. Researchers sorted genes by survival, immune features, expression in tumors versus normal brain, and validation in an outside cohort.
The funnel narrowed to six cancer-cell-predominant genes, then to three genes that were central in pathway and machine-learning analyses: PIK3CG, PRKCD, and TRIM22.
- PIK3CG: A phosphoinositide 3-kinase catalytic subunit with immune-signaling relevance.
- PRKCD: Protein kinase C delta type, a signaling enzyme linked to cell regulation and immune biology.
- TRIM22: A tripartite motif protein connected to immune response and cancer-related expression patterns.
The study’s central contrast is clinically uncomfortable: higher immune-activity markers did not necessarily point to longer survival in GBM.
Modern Glioblastoma Classification Changed the Validation Set
The TCGA source cohort was defined under older 2016 World Health Organization criteria. Current classification reserves the glioblastoma label for IDH-wildtype tumors, while IDH-mutant grade IV tumors are classified separately.
To match that modern definition, the analysis excluded 30 IDH-mutant astrocytoma cases and 123 cases with unknown IDH status. That left 372 IDH-wildtype GBM cases for the key clinicopathological validation.
- Discovery cohort: TCGA supplied 525 grade IV glioma cases with transcriptomic and survival data.
- Validation cohort: CGGA supplied 250 additional grade IV glioma cases.
- Normal comparator: GTEx supplied 1,152 normal brain tissue expression samples.
That classification step is important because mixed IDH status can blur GBM survival biology. IDH-mutant tumors often behave differently from IDH-wildtype glioblastoma.
High Gene Expression Tracked Poorer Overall Survival
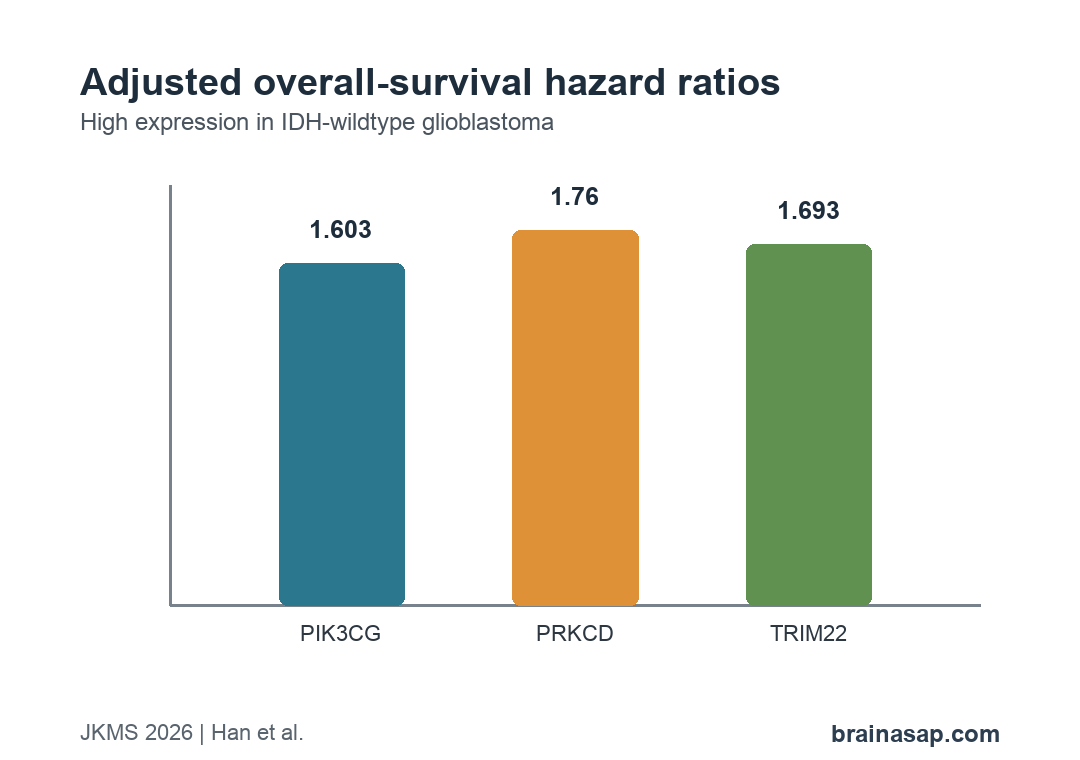
In the 372 IDH-wildtype GBM cases, high expression of all three genes was associated with poorer overall survival. The adjusted hazard ratios were 1.603 for PIK3CG, 1.760 for PRKCD, and 1.693 for TRIM22.
Disease-specific survival showed similar adjusted associations. Progression-free survival was less consistent; PIK3CG was significant in univariate analysis, while adjusted models for PRKCD and TRIM22 did not reach significance.
The immune data added a second layer. High expression of the three genes was also associated with immune-related features, including tumor-infiltrating lymphocyte measures and programmed death-ligand 1 expression patterns.
Machine Learning Added Prognostic Ranking but Not Mechanism
Two machine-learning approaches were used: adaptive elastic net regression and a gradient-boosting machine. These models helped rank gene contributions to survival prediction.
The adaptive elastic net model reported a 60-month AUC of 0.787. In the gradient-boosting model, SHAP values ranked PRKCD, RRAS2, PIK3CG, TRIM22, STAT5A, and CEPT1 as influential for survival probability.
The modeling was useful because GBM datasets contain many correlated measurements. A ranked model can help prioritize genes for laboratory work, but it cannot replace experiments that perturb the genes and measure tumor behavior.
- Prediction role: Machine learning helped identify which candidate genes held prognostic information in the dataset.
- Network role: Pathway analysis placed PIK3CG, PRKCD, and TRIM22 near immune and signaling clusters.
- Mechanism gap: Computational ranking does not prove that changing any one gene will alter GBM growth or immune response.
The study also used drug-sensitivity profiling to nominate possible therapeutic agents, including AGI-6780, linsitinib, and Nutlin-3a. Those findings should be read as screening leads, not treatment recommendations.
That distinction is especially important for GBM, where many promising computational or cell-line associations have not translated into effective patient therapies.
GBM Immunotherapy Interpretation Remains Complicated
GBM has been difficult for immunotherapy because the tumor microenvironment is often immunosuppressive. T-cell infiltration, interferon signaling, and checkpoint-related markers can coexist with poor outcomes.
That is why the three-gene result is notable. The genes were not simply “immune active equals good prognosis” markers; they were linked to immune activity and worse survival at the same time.
- Clinical use is premature: The markers are not ready for diagnosis, treatment selection, or prognosis in routine care.
- Biology needs testing: Cell, animal, and clinical validation would be needed to show causal roles.
- Combination idea: The findings support further study of chemotherapy and immune-based strategies, not immediate drug changes.
The most defensible reading is that PIK3CG, PRKCD, and TRIM22 deserve follow-up as GBM immune-prognostic markers. Their value will depend on whether experimental validation confirms that they are actionable rather than only correlated with aggressive tumors.
Citation: DOI: 10.3346/jkms.2026.41.e130. Han et al. Multi-Omics and Machine Learning Analyses Reveal PIK3CG, PRKCD, and TRIM22 as Potential Markers of Poor Prognosis and Immune Activation in Glioblastoma. Journal of Korean Medical Science. 2026;41:e130.
Study Design: Retrospective bioinformatics and machine-learning analysis of public glioblastoma transcriptomic datasets.
Sample Size: 525 TCGA grade IV glioma cases, 250 CGGA validation cases, 1,152 GTEx normal brain samples, and 372 IDH-wildtype GBM cases for focused validation.
Key Statistic: Adjusted overall-survival hazard ratios were 1.603 for PIK3CG, 1.760 for PRKCD, and 1.693 for TRIM22 in IDH-wildtype GBM.
Caveat: The study was computational and retrospective, so the three genes require mechanistic and clinical validation before use as therapeutic targets.