TL;DR: A 2026 study in Neurology found that higher autonomic symptom burden in moderate-advanced dementia with Lewy bodies was linked to worse cognitive fluctuations, higher neuropsychiatric burden, and lower caregiver quality of life over time.
Key Findings
- Autonomic burden was measured longitudinally across 189 people with moderate-advanced dementia with Lewy bodies.
- Higher Autonomic Symptom Checklist scores predicted worse Clinician Assessment of Fluctuations scores over time.
- Neuropsychiatric Inventory-Questionnaire scores also rose as autonomic symptom burden increased.
- Caregiver quality of life was lower when autonomic burden was higher in longitudinal adjusted models.
- The study was observational, so it cannot prove that treating autonomic symptoms would reduce cognitive or psychiatric symptoms.
Source: The analysis used data from the PACE-DLB cohort, a U.S. longitudinal study of people with moderate-advanced dementia with Lewy bodies and their primary caregivers.
Autonomic Symptoms Tracked With Cognitive Fluctuations in Lewy Body Dementia
Dementia with Lewy bodies (DLB) can involve memory and thinking problems, hallucinations, movement changes, sleep disturbance, and swings in attention. One of its difficult features is cognitive fluctuation: a person’s alertness or thinking can worsen for minutes or hours, then partly improve again.
The Neurology study focused on whether these fluctuations travel with dysautonomia, meaning problems in automatic body functions such as blood pressure control, gastrointestinal symptoms, temperature regulation, sweating, and other peripheral symptoms.
Researchers measured dysautonomia with the Autonomic Symptom Checklist (ASC), a 19-item symptom count used in Lewy body disease.
The main result was consistent across baseline and follow-up data: people with more autonomic symptoms tended to have worse fluctuation scores and more neuropsychiatric symptoms.
- Cognitive fluctuations: Higher ASC scores were associated with higher Clinician Assessment of Fluctuations scores.
- Neuropsychiatric burden: Higher ASC scores were associated with higher Neuropsychiatric Inventory-Questionnaire scores.
- Caregiver quality of life: Higher ASC scores were linked with lower caregiver-reported quality of life over time.
Autonomic symptoms are often treated as separate non-motor problems. This analysis suggests they may also mark a broader symptom cluster in advanced DLB.
PACE-DLB Followed 189 Patient-Caregiver Dyads
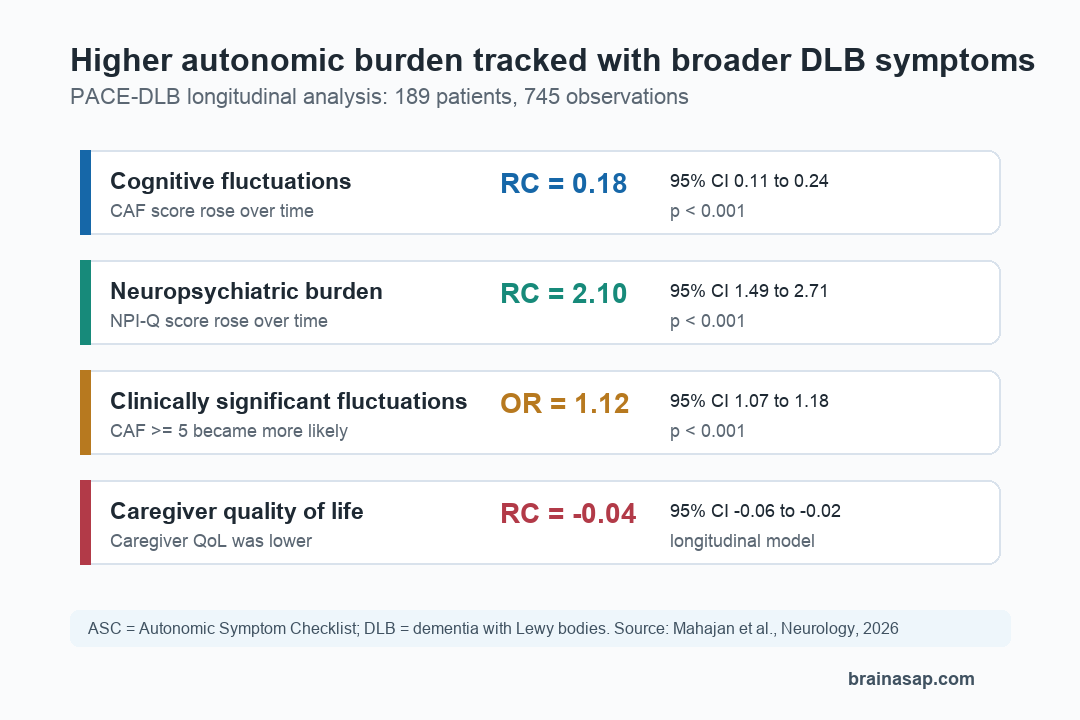
The analysis included 189 patients and 745 longitudinal observations. Participants had moderate-advanced DLB and were followed through the Predicting ACcurately End-of-Life in Dementia with Lewy Bodies and Promoting Quality End-of-Life Experiences study, abbreviated PACE-DLB.
Recruitment came from five Lewy Body Dementia Association Research Centers of Excellence and a virtual cohort outside subspecialty care. Study visits occurred every 6 months, mostly by telephone or secure video, with coordinators administering the measures.
At baseline, the average participant was 74.9 years old, and the cohort was 22.2% female. The average Autonomic Symptom Checklist score was 8.06 out of 19, reflecting a substantial symptom load in this moderate-advanced group.
- Exposure: Autonomic burden measured by the Autonomic Symptom Checklist.
- Main cognitive outcome: Clinician Assessment of Fluctuations (CAF), a brief interview scale for fluctuation frequency and duration.
- Main psychiatric outcome: Neuropsychiatric Inventory-Questionnaire (NPI-Q), a measure of symptoms such as agitation, hallucinations, depression, anxiety, sleep disturbance, and apathy.
- Quality-of-life outcome: Quality of Life-Alzheimer’s Disease ratings for the patient, informant view of the patient, and caregiver.
Researchers adjusted the analyses for age, sex, education, comorbidity, anticholinergic burden, levodopa-equivalent dose, and daytime sleepiness. They also ran longitudinal mixed-effects models and network analyses to check whether the pattern held over repeated visits.
Higher ASC Scores Predicted Worse CAF and NPI-Q Scores
At baseline, total autonomic burden was associated with worse fluctuation scores after adjustment. Each higher ASC point corresponded to a 0.16-point higher CAF score (95% CI, 0.01 to 0.31; p=0.032).
The neuropsychiatric association was larger. At baseline, each higher ASC point corresponded to a 3.27-point higher NPI-Q score (95% CI, 2.37 to 4.18; p<0.001), after adjustment.
The longitudinal models showed the same direction over time:
- CAF over time: ASC remained associated with cognitive fluctuations (RC=0.18; 95% CI, 0.11 to 0.24; p<0.001).
- NPI-Q over time: ASC remained associated with neuropsychiatric burden (RC=2.10; 95% CI, 1.49 to 2.71; p<0.001).
- Clinically significant fluctuations: Greater autonomic burden was associated with higher odds of clinically significant cognitive fluctuations, defined as CAF at least 5 (OR=1.12; 95% CI, 1.07 to 1.18; p<0.001).
A network model also kept the same relationships visible. Total ASC was linked with neuropsychiatric burden with a network weight of 0.47 and with cognitive fluctuations with a network weight of 0.15.
Different Autonomic Domains Pointed to Different Symptom Patterns
The total ASC score was not the only signal. When researchers separated autonomic symptoms into domains, different symptom groups lined up with different outcomes.
Cardiovascular autonomic burden was most clearly tied to cognitive fluctuations. In longitudinal analysis, cardiovascular symptoms were associated with CAF scores (RC=0.51; 95% CI, 0.23 to 0.78; p<0.001), but not with neuropsychiatric burden.
Gastrointestinal and thermoregulatory symptoms were more closely tied to neuropsychiatric burden. So were peripheral autonomic symptoms. In longitudinal models, GI/thermoregulatory burden and peripheral burden both correlated with NPI-Q scores.
- Attention and alertness: Cardiovascular symptoms may fit with episodes of reduced brain perfusion, blood-pressure instability, or arousal-system disruption.
- Psychiatric and behavioral symptoms: GI, thermoregulatory, and peripheral symptoms may reflect broader autonomic involvement that travels with distress, sleep problems, hallucinations, or agitation.
- Caregiver burden: Neuropsychiatric symptoms partly explained the link between autonomic burden and lower caregiver quality of life.
The study does not show that one symptom domain causes another.
Autonomic burden was not just a background feature in this cohort. It tracked with the symptoms families often experience as most disruptive.
The Main Limit Is Causality
The strongest boundary is that the analysis was observational. Researchers could adjust for measured confounders, but they could not prove that dysautonomia caused worse cognitive fluctuations or psychiatric symptoms.
The autonomic measure was also caregiver-reported rather than based on standardized objective autonomic testing. That choice captured symptoms across a large, seriously affected group, but it may miss physiological details such as orthostatic blood pressure changes.
Diagnosis was another boundary. Participants had a clinical DLB diagnosis supported by the Lewy Body Composite Risk Score, but the study could not confirm that every participant met formal possible or probable DLB criteria.
For moderate-advanced DLB care, autonomic symptoms may deserve closer attention when clinicians and caregivers are trying to understand sudden shifts in alertness, behavioral symptoms, and caregiver strain.
Citation: DOI: 10.1212/WNL.0000000000214934. Mahajan et al. Cognitive fluctuations, neuropsychiatric burden and quality of life in moderate-advanced dementia with Lewy bodies: the role of dysautonomia. Neurology. 2026;106:e214934.
Study Design: Multi-center prospective observational longitudinal cohort analysis of moderate-advanced dementia with Lewy bodies.
Sample Size: 189 patients and primary caregivers, contributing 745 longitudinal observations.
Key Statistic: Longitudinal ASC scores were associated with CAF scores (RC=0.18) and NPI-Q scores (RC=2.10), both p<0.001.
Caveat: The study used caregiver-reported autonomic symptoms and cannot prove that treating dysautonomia would reduce cognitive fluctuations or neuropsychiatric symptoms.





