TL;DR: A 2026 study in Brain, Behavior, & Immunity – Health linked better sleep quality before influenza vaccination and earlier chronotype to stronger immune-response markers in 108 adults.
Key Findings
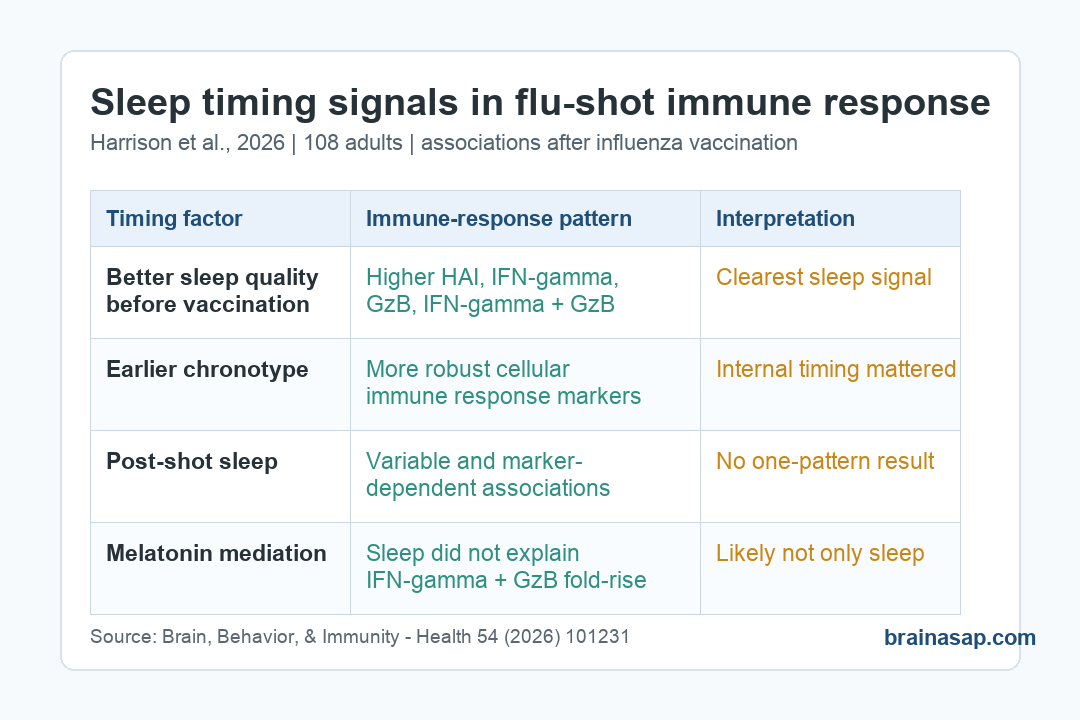
- Vaccination cohort: Researchers studied sleep, vaccination timing, chronotype, and immune markers in 108 adults after influenza vaccination.
- Pre-shot sleep quality: Better Pittsburgh Sleep Quality Index sleep-quality scores before vaccination were linked to stronger HAI, IFN-gamma, granzyme B, and combined IFN-gamma + granzyme B responses.
- Earlier chronotype: Morning-leaning chronotype was associated with more robust cellular immune responses across multiple measures.
- Post-shot sleep: Sleep after vaccination showed more variable, marker-specific associations rather than one clean pattern.
- Main caveat: The trial was a pilot analysis, so it supports sleep and circadian timing as vaccine-response variables, not as proven clinical instructions.
Source: Harrison et al. 2026.
Sleep around vaccination is usually discussed as a general wellness habit. This study tested a sharper question: whether sleep quality, sleep timing, chronotype, and vaccination timing line up with measurable immune responses after a flu shot.
The findings do not support a simple “sleep more after the shot” message. The clearest sleep association appeared before vaccination, while the timing of a person’s internal clock added another layer.
Better Pre-Vaccination Sleep Quality Tracked With Stronger Immune Markers
Researchers analyzed 108 adults in the Melatonin and Vaccine Response Immunity and Chronobiology Study, or MAVRICS. Participants received influenza vaccination and were followed with sleep measures, timing measures, and immune assays about 2 weeks later.
The main sleep association came from pre-vaccination sleep quality, measured with the Pittsburgh Sleep Quality Index. On that scale, lower values indicate better sleep quality.
After adjustment for sex, age, treatment group, and baseline immune levels, better sleep quality before vaccination was associated with stronger immune responses. The linked markers included:
- HAI titers: Hemagglutination inhibition titers for the Victoria influenza lineage, a standard antibody-related vaccine-response measure.
- IFN-gamma: Interferon gamma, an immune signaling protein involved in antiviral cellular responses.
- Granzyme B: A cytotoxic-cell enzyme that helps immune cells kill infected or abnormal cells.
- Dual response: Combined IFN-gamma + granzyme B activity, a cellular response marker reported in the earlier melatonin analysis.
All of those pre-vaccination sleep-quality associations were reported at p < 0.05. The study does not prove that improving sleep quality before vaccination will automatically improve vaccine protection, but it does make the pre-shot window biologically plausible.
Chronotype Looked More Important Than Clock Time Alone
Chronotype describes preferred sleep-wake timing. Earlier chronotypes tend to function better earlier in the day, while later chronotypes tend to shift sleep and activity later.
In this study, earlier chronotype was associated with more robust cellular immune response across multiple measures. Vaccination timing is often described by wall-clock time, such as morning versus afternoon, but internal timing may carry additional information.
The study separated several timing concepts that can be easy to merge:
- Clock time of vaccination: The external appointment time, which ranged from 08:22 to 18:30 in the sample.
- Circadian timing of vaccination: The appointment time estimated relative to the participant’s internal biological timing.
- Chronotype: The participant’s usual sleep-wake preference, measured with the Munich Chronotype Questionnaire.
- Social jetlag: The mismatch between workday and free-day sleep timing.
The strongest discussion point was that chronotype, not just clock time, may help explain why some vaccination-time studies find morning advantages and others do not. A morning appointment may not mean the same biological time for every person.
Post-Vaccination Sleep Was More Mixed
The post-shot sleep story was less clean. Actigraphy showed average post-vaccination sleep durations of 7 hours 4 minutes in the melatonin group and 6 hours 55 minutes in controls.
The melatonin group had shorter sleep onset latency on the first night after vaccination: 8.02 minutes versus 12.96 minutes in controls, with p = 0.046. Sleep onset latency means how long it took to fall asleep.
Even so, mediation analyses did not show that sleep explained the previously reported melatonin-related increase in IFN-gamma + granzyme B fold-rise. Direct and indirect sleep-mediated paths were not significant.
That distinction keeps the interpretation narrower. Melatonin may have immune effects that are not simply a byproduct of better sleep in this dataset.
The Immune Measures Captured Different Parts of Vaccine Response
Influenza vaccine response is not a single number. The study measured antibody-related response and cellular response, which can move differently.
The main immune readouts included:
- HAI titers: A blood test that estimates how well antibodies block influenza hemagglutinin activity.
- Fluorospot IFN-gamma: A cellular assay showing immune-cell signaling after antigen stimulation.
- Granzyme B response: A marker tied to cytotoxic immune activity.
- Fold-rise: The change from baseline to the post-vaccination measurement window.
Because these markers reflect different immune functions, the mixed post-vaccination sleep findings are not surprising. A sleep variable can line up with one immune endpoint while showing little association with another.
This Is a Timing Signal, Not a Vaccine Schedule Rule
The study is useful because sleep quality and circadian timing are potentially modifiable. They are also measurable, which means future vaccine studies can stop treating “morning appointment” as a one-size timing variable.
Still, the clinical message should stay narrow. The study was not designed to assign people to sleep-improvement programs before vaccination, and it did not test whether changing chronotype changes vaccine response.
The practical takeaway is more disciplined: when researchers study vaccine response, they should measure pre-vaccination sleep quality, chronotype, and internal biological timing instead of relying only on clock time.
The result supports a low-risk common-sense behavior: do not treat the night before vaccination as irrelevant. Better sleep quality before the shot may be part of the immune-response context, even though it is not a substitute for vaccination, medical guidance, or risk-based vaccine timing.
Citation: DOI: 10.1016/j.bbih.2026.101231. Harrison et al. Influenza vaccine response is predicted by chronotype and differentially associated with pre- and post-vaccination sleep. Brain, Behavior, & Immunity – Health. 2026;54:101231.
Study Design: Pilot analysis of sleep, circadian timing, melatonin assignment, and immune response after influenza vaccination.
Sample Size: 108 adults, with blood draws about 2 weeks after vaccination and sleep/timing measures around vaccination.
Key Statistic: Better pre-vaccination sleep quality was associated with higher Victoria-lineage HAI titers and elevated IFN-gamma, granzyme B, and IFN-gamma + granzyme B responses, all p < 0.05.
Caveat: Associations do not prove that changing sleep quality or chronotype will causally improve vaccine response.